
Polycystic Ovary Syndrome (PCOS) remains the leading cause of anovulatory infertility and the most prevalent endocrine disorder among women of reproductive age globally. As clinical understanding of the condition has evolved, the focus of treatment has shifted significantly toward addressing underlying metabolic dysfunction, specifically insulin resistance. Among the various therapeutic interventions available, two substances—the pharmaceutical agent metformin and the naturally occurring carbohydrate inositol—have emerged as the primary contenders for managing the syndrome’s complex symptom profile. While both act as insulin sensitizers, their mechanisms, side-effect profiles, and long-term implications present distinct choices for patients and healthcare providers.
The Pathophysiological Link Between Insulin and PCOS
To understand the comparative utility of metformin and inositol, it is necessary to examine the metabolic framework of PCOS. Research indicates that approximately 75% of women with PCOS exhibit some degree of insulin resistance, regardless of their body mass index (BMI). In these individuals, the body’s cells become less responsive to insulin, the hormone responsible for regulating blood glucose levels. Consequently, the pancreas compensates by overproducing insulin, leading to hyperinsulinemia.

This excess insulin acts as a primary driver of PCOS symptoms through several pathways. First, high insulin levels stimulate the theca cells in the ovaries to produce excessive amounts of androgens, such as testosterone. Second, it suppresses the production of Sex Hormone-Binding Globulin (SHBG) in the liver, which further increases the amount of free, active testosterone in the bloodstream. These hormonal imbalances lead to the hallmark symptoms of the condition: irregular menstrual cycles, hirsutism (excessive hair growth), acne, and weight gain, particularly in the abdominal region. By improving the body’s sensitivity to insulin, both metformin and inositol aim to break this cycle of hormonal overproduction.
Metformin: The Pharmaceutical Standard
Metformin, a biguanide originally derived from the French lilac plant, has been a cornerstone in the treatment of Type 2 diabetes for decades. Its adoption for PCOS management began in the late 1990s as clinicians observed its ability to lower androgen levels and restore ovulation in insulin-resistant patients.
The drug functions through three primary mechanisms. It reduces the amount of glucose produced by the liver (gluconeogenesis), decreases the absorption of glucose in the intestines, and increases the sensitivity of peripheral tissues—specifically skeletal muscle—to insulin. On a cellular level, metformin activates the enzyme adenosine monophosphate-activated protein kinase (AMPK), which plays a crucial role in cellular energy homeostasis.

Clinical data supports the efficacy of metformin in the PCOS population. Studies have demonstrated that it can effectively lower fasting blood sugar, reduce androgen levels, and improve the frequency of ovulation. However, its impact on weight loss remains a subject of debate. While some patients experience moderate weight reduction, a 2000 study published in the journal PubMed noted that many women showed little change in their BMI even after six months of consistent use.
Inositol: The Emergence of Nutraceutical Alternatives
Inositol, often referred to as Vitamin B8 (though technically a sugar alcohol), is found naturally in fruits, beans, grains, and nuts. In the context of PCOS, two specific isomers—myo-inositol (MI) and d-chiro-inositol (DCI)—are of particular clinical interest. These molecules act as secondary messengers in the insulin signaling pathway.
The mechanism of inositol is often described using a "lock and key" analogy. For insulin to function, it must bind to a receptor on the cell wall. Inositol is integral to the internal signaling that occurs once that bond is made. It helps the "lock" work more efficiently, ensuring that the cell opens to glucose without requiring excessive insulin. Furthermore, inositol is involved in the signaling of the Follicle-Stimulating Hormone (FSH), which is vital for egg development and ovulation.

A systematic review and meta-analysis published in the European Review compared the effects of myo-inositol and metformin. The findings indicated that myo-inositol was comparable to metformin in improving insulin resistance, reducing androgen levels, and increasing pregnancy rates. Crucially, inositol appeared to offer superior results in improving egg quality, a factor that is particularly relevant for women undergoing assisted reproductive technologies (ART) like IVF.
A Chronology of Clinical Adoption and Research
The timeline of these treatments reflects a broadening of the medical approach to PCOS:
- 1994–1998: Initial studies suggest that metformin, by lowering insulin, could potentially treat the reproductive symptoms of PCOS.
- 2000: Randomized double-blind trials establish metformin’s role in improving metabolic profiles, though weight loss benefits are found to be inconsistent.
- 2010: Research begins to focus heavily on myo-inositol as a safer, "natural" alternative with a lower side-effect profile.
- 2013–2017: Comparative studies show that myo-inositol is not only as effective as metformin for many patients but may also be superior in restoring regular menstrual cycles and improving oocyte quality.
- 2021–Present: The medical community increasingly recognizes the "40:1 ratio" (myo-inositol to d-chiro-inositol) as the physiological standard for optimal PCOS management, leading to the popularity of combination supplements like Ovasitol.
Comparative Data: Efficacy and Patient Compliance
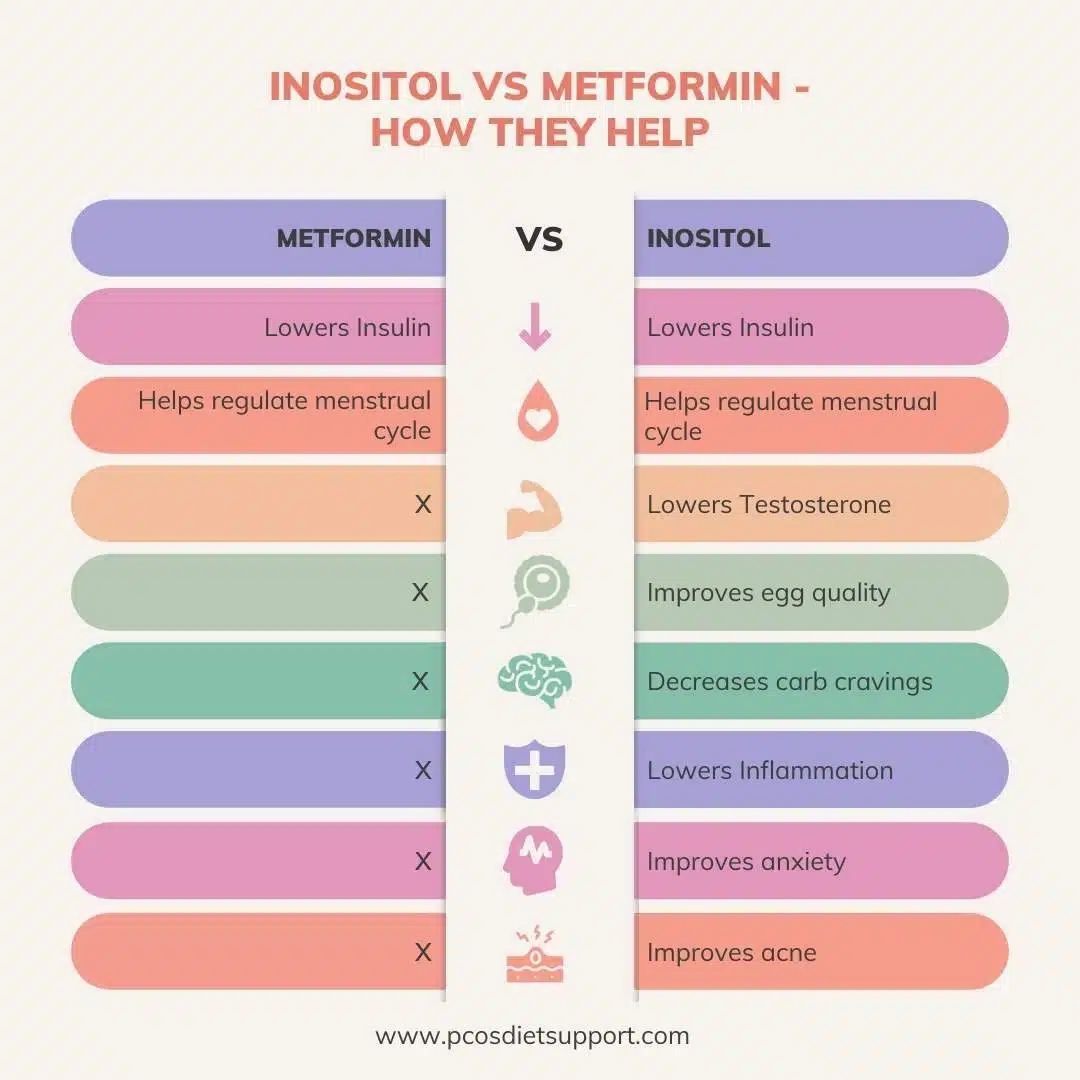
When evaluating the two treatments side-by-side, the data reveals significant overlap in benefits but a stark divergence in patient experience. Both substances are proven to lower testosterone, improve skin health, and help regulate the menstrual cycle. However, the side-effect profile of metformin is a major barrier to patient compliance.

Metformin is notorious for causing gastrointestinal distress, including nausea, diarrhea, and abdominal cramping. Long-term use has also been linked to Vitamin B12 deficiency, necessitating regular monitoring. In rare cases, it can lead to lactic acidosis, a serious medical condition.
In contrast, inositol is generally well-tolerated. The most common side effects are mild digestive upset or occasional headaches, which often resolve by adjusting the timing of the dose or taking it with food. Because inositol is a substance already present in the human body, the risk of severe adverse reactions is significantly lower. This higher tolerability often leads to better long-term adherence to the treatment protocol.
Official Responses and Clinical Perspectives
Medical professionals, such as registered dietitians specializing in PCOS, often advocate for a nuanced approach. Angela Grassi, a leading expert in PCOS nutrition, notes that while metformin is a powerful tool, it is not a "magic pill" for weight loss. The consensus among many specialists is that the choice between the two should be individualized based on the patient’s specific symptoms, metabolic labs, and fertility goals.

While some physicians remain hesitant to prescribe supplements over traditional pharmaceuticals, the growing body of peer-reviewed evidence for inositol has led to its inclusion in many clinical guidelines. Some practitioners now suggest a combination therapy, where lower doses of both metformin and inositol are used to maximize insulin sensitivity while minimizing the gastrointestinal side effects associated with high-dose metformin.
Broader Impact and Implications for Women’s Health
The debate between inositol and metformin highlights a larger trend in modern medicine: the shift toward integrative health. For the millions of women living with PCOS, the availability of an over-the-counter supplement that rivals a prescription drug in efficacy is a significant development. It empowers patients who may be wary of pharmaceutical side effects or who lack easy access to specialized endocrine care.
Furthermore, the focus on insulin sensitizers underscores the fact that PCOS is not merely a "fertility issue" but a lifelong metabolic condition. Managing insulin levels early in life can reduce the long-term risk of developing Type 2 diabetes, cardiovascular disease, and endometrial cancer.
In conclusion, while metformin remains a validated and effective treatment with decades of research behind it, inositol has proven itself to be a formidable alternative. With its high safety profile and specific benefits for egg quality and cycle regularity, inositol is increasingly viewed as a first-line intervention. As research continues to emerge, the medical community is likely to move toward a more flexible model of care that prioritizes patient comfort and metabolic health in equal measure. Women are advised to consult with their healthcare providers to determine which insulin sensitizer—or combination thereof—aligns best with their unique physiological needs and long-term health objectives.
