
Polycystic Ovary Syndrome (PCOS) remains the most prevalent endocrine disorder among women of reproductive age globally, affecting an estimated 8% to 13% of the female population. Characterized by hormonal imbalances, irregular menstrual cycles, and the presence of small cysts on the ovaries, the condition is deeply intertwined with metabolic dysfunction. Central to the pathology of PCOS is insulin resistance, a condition where the body’s cells do not respond effectively to insulin, leading the pancreas to overproduce the hormone. This state of hyperinsulinemia triggers the ovaries to produce excess androgens, such as testosterone, which further exacerbates symptoms like acne, hirsutism, and ovulatory dysfunction. To manage these symptoms, medical professionals frequently turn to insulin sensitizers, with the pharmaceutical agent Metformin and the nutritional supplement Inositol being the two primary contenders. As clinical research evolves, the debate over which intervention offers the most favorable balance of efficacy and tolerability has become a focal point for reproductive endocrinology.
The Role of Insulin Sensitizers in PCOS Management
The physiological link between insulin and reproductive health is the primary reason why insulin-sensitizing agents are considered a cornerstone of PCOS therapy. In women with PCOS, insulin resistance is present in up to 75% of cases, regardless of Body Mass Index (BMI), though obesity can significantly worsen the condition. When insulin levels remain chronically elevated, they suppress the production of Sex Hormone-Binding Globulin (SHBG) in the liver. Lower levels of SHBG mean there is more "free" or active testosterone circulating in the bloodstream, leading to the androgenic symptoms typical of the syndrome.

By improving the body’s sensitivity to insulin, both Metformin and Inositol aim to break this cycle. The objective is to lower circulating insulin levels, thereby reducing androgen production, restoring regular ovulation, and mitigating the long-term risks associated with PCOS, such as Type 2 diabetes and cardiovascular disease.
Metformin: The Pharmaceutical Gold Standard
Metformin, a biguanide derivative originally sourced from the French lilac plant, has been a staple in the treatment of Type 2 diabetes for decades. Its application in PCOS management, though often categorized as "off-label" in several jurisdictions, is supported by a vast body of clinical evidence. Metformin primarily functions through three distinct mechanisms: it inhibits glucose production in the liver (gluconeogenesis), decreases the intestinal absorption of glucose, and enhances peripheral glucose uptake by increasing the sensitivity of muscle cells to insulin.
Clinical data, including a landmark study published in the journal Human Reproduction Update, confirms that Metformin can significantly improve ovulation rates in women with PCOS. By lowering insulin, Metformin helps recalibrate the Hypothalamic-Pituitary-Ovarian (HPO) axis. However, the drug is not without its limitations. While it is highly effective at managing blood sugar and reducing androgen levels, its impact on weight loss is often described as modest. In a six-month randomized, double-blind, placebo-controlled trial, researchers noted that while metabolic profiles improved, many participants showed little to no change in their BMI.

Furthermore, Metformin is notorious for its gastrointestinal side effects. Clinical reports indicate that up to 30% of patients experience nausea, diarrhea, abdominal cramping, or vomiting, particularly during the initial weeks of treatment. Long-term use has also been linked to Vitamin B12 deficiency, necessitating regular monitoring and supplementation for many women.
Inositol: The Emergence of a Natural Alternative
Inositol, often referred to as Vitamin B8 (though it is technically a carbocyclic sugar), has gained significant traction as a first-line alternative to Metformin. Found naturally in fruits, beans, grains, and nuts, inositol exists in several forms, with Myo-inositol (MI) and D-chiro-inositol (DCI) being the most relevant to PCOS. These molecules act as "second messengers" in the insulin signaling pathway.
When insulin binds to a cell receptor, inositol-containing compounds are responsible for relaying the signal into the cell to activate glucose transporters. In women with PCOS, there is often a defect in this signaling pathway, or an imbalance in the ratio of MI to DCI within the follicular fluid of the ovaries. Myo-inositol is particularly crucial for the activation of Follicle-Stimulating Hormone (FSH) signals, which are essential for egg development and quality.

A 2021 systematic review and meta-analysis published in European Review for Medical and Pharmacological Sciences compared the effects of Myo-inositol and Metformin. The analysis concluded that Myo-inositol was essentially as effective as Metformin in improving insulin sensitivity and reducing androgen levels. Crucially, inositol appeared to offer superior results regarding egg quality and a lower risk of ovarian hyperstimulation syndrome (OHSS) in women undergoing assisted reproductive technologies.
Comparative Chronology and Clinical Evolution
The transition from Metformin-dominance to the consideration of Inositol has followed a clear chronological path in medical literature:
- 1990s – Early 2000s: Metformin becomes the primary tool for managing PCOS-related insulin resistance following successful trials in diabetic populations.
- Mid-2000s: Research begins to highlight the high dropout rates of Metformin users due to gastrointestinal distress.
- 2008 – 2012: Initial studies on Myo-inositol demonstrate its ability to restore spontaneous ovarian activity and improve fertility.
- 2013 – 2019: The "40:1 Ratio" theory gains prominence, suggesting that a specific combination of Myo-inositol and D-chiro-inositol mimics the body’s natural balance and provides optimal results for PCOS patients.
- 2020 – Present: Comparative trials increasingly suggest that while both are effective, Inositol’s safety profile makes it a more sustainable long-term option for many.
Side Effect Profiles and Patient Compliance
One of the most significant factors in the Metformin versus Inositol debate is patient compliance. The therapeutic dose of Metformin typically ranges from 1,500mg to 2,000mg per day. For many women, reaching this dose is a process of "trial and error" fraught with digestive upset. In contrast, Inositol is generally well-tolerated. The most common side effects are mild digestive changes or occasional headaches, which usually resolve as the body adjusts.

The "Metformin Fatigue" phenomenon—where patients discontinue treatment due to a diminished quality of life caused by chronic nausea—has led many practitioners to lead with Inositol. Additionally, because Inositol is a naturally occurring sugar alcohol, it does not carry the rare but serious risk of lactic acidosis associated with Metformin in patients with renal or hepatic impairment.
Synergistic Effects: Can They Be Taken Together?
A growing area of interest for endocrinologists is the combination of both Metformin and Inositol. Because they work on slightly different aspects of the insulin signaling pathway—Metformin primarily through the AMPK pathway and Inositol through the inositolphosphoglycan (IPG) second messenger system—there is a theoretical synergy.
Recent studies have explored whether combining a lower dose of Metformin with Inositol can achieve the same metabolic benefits as a high dose of Metformin alone, but with significantly fewer side effects. Preliminary results are promising, showing that combination therapy can lead to better outcomes in menstrual regularity and weight management than either treatment used in isolation. However, medical experts warn that combining two insulin-sensitizing agents increases the risk of hypoglycemia (low blood sugar), and such a regimen should only be undertaken under strict medical supervision.

Broader Implications and Long-term Outlook
The choice between Metformin and Inositol is not merely about managing current symptoms; it is about long-term disease prevention. Women with PCOS have a significantly higher risk of developing gestational diabetes during pregnancy and Type 2 diabetes later in life.
Metformin has a longer track record in preventing the progression to Type 2 diabetes in high-risk populations. However, Inositol’s ability to improve lipid profiles—specifically lowering triglycerides and improving the LDL/HDL cholesterol ratio—gives it a distinct advantage in managing cardiovascular risk.
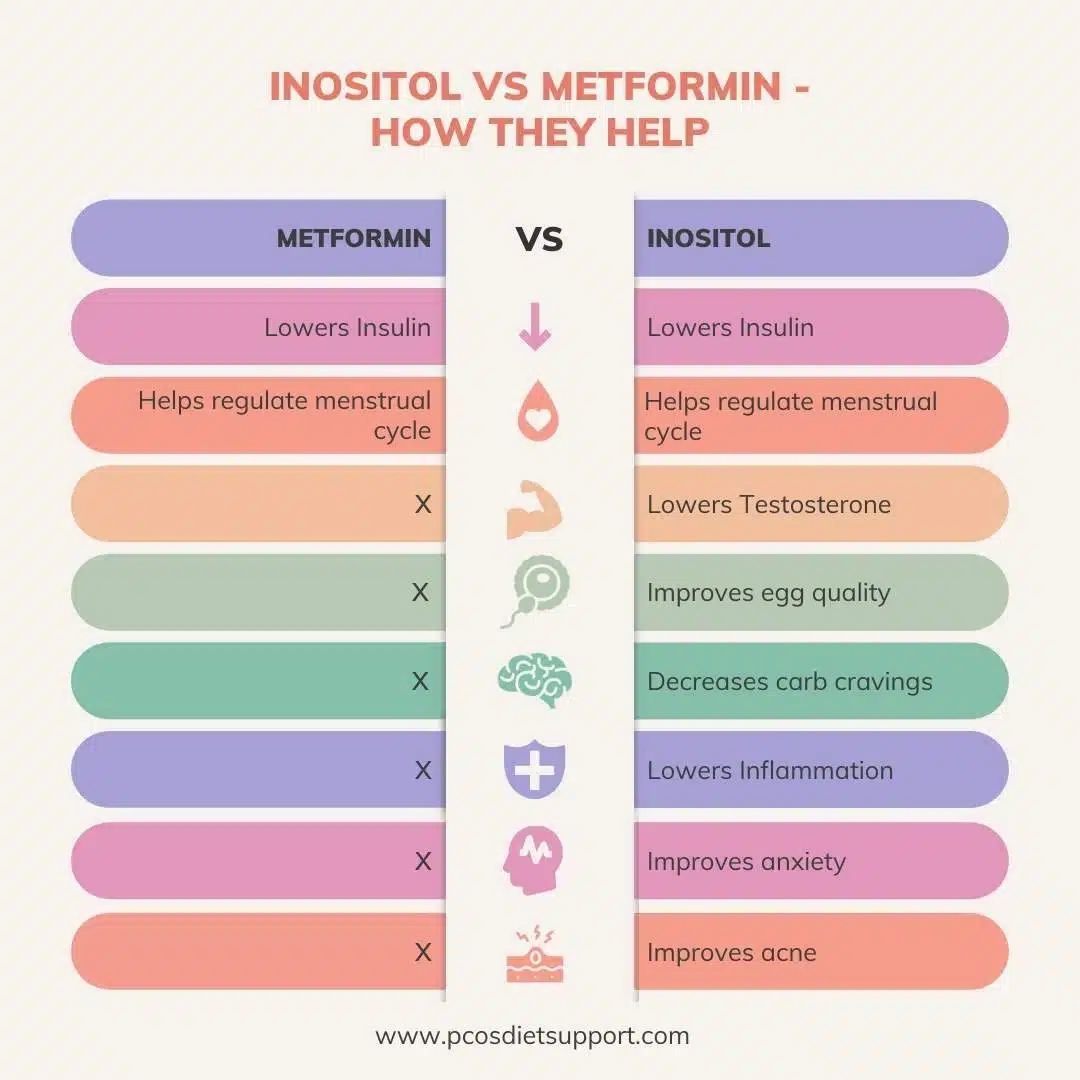
From a journalistic and clinical perspective, the "better" option is often determined by the patient’s specific goals. If the primary goal is rapid stabilization of high blood sugar in a clinical diabetic range, Metformin remains a powerful pharmaceutical tool. If the goal is fertility, egg quality, and long-term management with minimal side effects, Inositol is increasingly viewed as the preferred choice.
Conclusion
The comparative analysis of Inositol and Metformin reveals that while both agents are highly effective at addressing the root cause of PCOS—insulin resistance—their paths to achieving that goal differ. Metformin offers a potent, well-researched pharmaceutical approach but is hampered by significant side effects. Inositol provides a "gentler" alternative that matches Metformin’s efficacy in many areas while offering additional benefits for reproductive health and egg quality. As personalized medicine continues to evolve, the integration of these treatments, tailored to the individual metabolic and reproductive needs of the patient, will likely become the standard of care in the management of Polycystic Ovary Syndrome.
