
The medical community has long recognized Polycystic Ovary Syndrome (PCOS) as the leading endocrine disorder among women of reproductive age, yet the debate over the most effective metabolic intervention remains a focal point of clinical research. Central to this discussion is the comparison between Metformin, a venerable pharmaceutical staple for type 2 diabetes, and Inositol, a naturally occurring sugar alcohol that has gained significant traction as a nutraceutical alternative. As clinical evidence suggests that insulin resistance affects up to 75% of women diagnosed with PCOS, the choice between these two insulin-sensitizing agents carries profound implications for symptom management, fertility outcomes, and long-term metabolic health.
The Metabolic Foundation of PCOS
To understand the competition between Inositol and Metformin, one must first address the underlying pathophysiology of PCOS. While the condition is often characterized by its outward symptoms—such as irregular menstrual cycles, hirsutism, and acne—its "engine" is frequently metabolic. Insulin resistance occurs when the body’s cells become less responsive to the hormone insulin, which is responsible for regulating blood glucose levels. In response, the pancreas secretes higher volumes of insulin to compensate.

This state of hyperinsulinemia triggers the ovaries to produce excess androgens, particularly testosterone. High androgen levels interfere with the maturation of follicles, leading to the "cysts" (underdeveloped follicles) observed in ultrasound scans and the subsequent failure to ovulate. Furthermore, excess insulin decreases the production of Sex Hormone-Binding Globulin (SHBG), which normally binds to testosterone to keep it inactive in the bloodstream. Consequently, the management of insulin levels has become a primary target for clinicians seeking to restore hormonal balance.
Metformin: The Pharmaceutical Gold Standard
Metformin has served as the first-line defense for metabolic dysfunction for decades. Originally derived from the French lilac, it was approved in the United States in the mid-1990s for type 2 diabetes and soon after found "off-label" utility in the treatment of PCOS. Its primary function is to suppress glucose production in the liver and improve the sensitivity of peripheral tissues—such as muscle and fat—to existing insulin.
According to clinical guidelines, Metformin operates through three distinct pathways. First, it inhibits gluconeogenesis, the process by which the liver creates new glucose. Second, it slows the absorption of carbohydrates in the intestinal tract. Third, it activates an enzyme called AMPK (adenosine monophosphate-activated protein kinase), which plays a crucial role in cellular energy homeostasis. Research published in the journal Human Reproduction indicates that Metformin can effectively lower androgen levels and restore regular menstrual cycles in approximately 50% to 70% of patients. However, its impact on weight loss remains modest; while it prevents further weight gain, many clinical trials show only negligible reductions in Body Mass Index (BMI) after six months of therapy.

Inositol: The Emerging Nutraceutical Alternative
Inositol, often referred to as Vitamin B8 (though it is technically a sugar alcohol), represents a different approach to insulin sensitization. It is found naturally in fruits, beans, grains, and nuts, and the human body also synthesizes it from glucose. In the context of PCOS, two specific isomers are of interest: Myo-inositol (MI) and D-chiro-inositol (DCI).
The mechanism of Inositol is inherently cellular. It acts as a "second messenger" in the insulin signaling pathway. When insulin binds to a cell receptor, Inositol-containing molecules (phosphoglycans) are released to trigger the actual uptake of glucose. In many women with PCOS, there appears to be a defect in this "lock and key" mechanism. Supplementation with Inositol bypasses this defect, allowing the cell to respond to insulin more efficiently. A landmark study published in the European Review for Medical and Pharmacological Sciences compared Myo-inositol directly to Metformin and found that Inositol was not only as effective in improving insulin sensitivity but also superior in terms of patient compliance and reduction in side effects.
A Chronology of Treatment Evolution
The shift from purely hormonal treatments to metabolic interventions reflects a broader evolution in the understanding of PCOS.

- 1935: Doctors Stein and Leventhal first describe the syndrome, focusing primarily on the physical appearance of the ovaries.
- 1980s: Research begins to link PCOS with hyperinsulinemia and a higher risk of gestational diabetes.
- 1994: Metformin enters the U.S. market, and clinicians begin experimenting with its use for non-diabetic PCOS patients.
- 2000s: Early studies on Inositol emerge from Italy, suggesting that Myo-inositol can restore ovulation without the gastrointestinal distress associated with pharmaceuticals.
- 2010s: The "40:1 ratio" (Myo-inositol to D-chiro-inositol) is identified as the physiological plasma ratio, leading to the development of specialized supplements like Ovasitol.
- 2020-Present: Large-scale meta-analyses confirm that Inositol and Metformin have comparable efficacy in many areas, though Inositol is increasingly preferred for fertility-focused patients due to its positive impact on oocyte (egg) quality.
Comparative Data: Efficacy and Side Effects
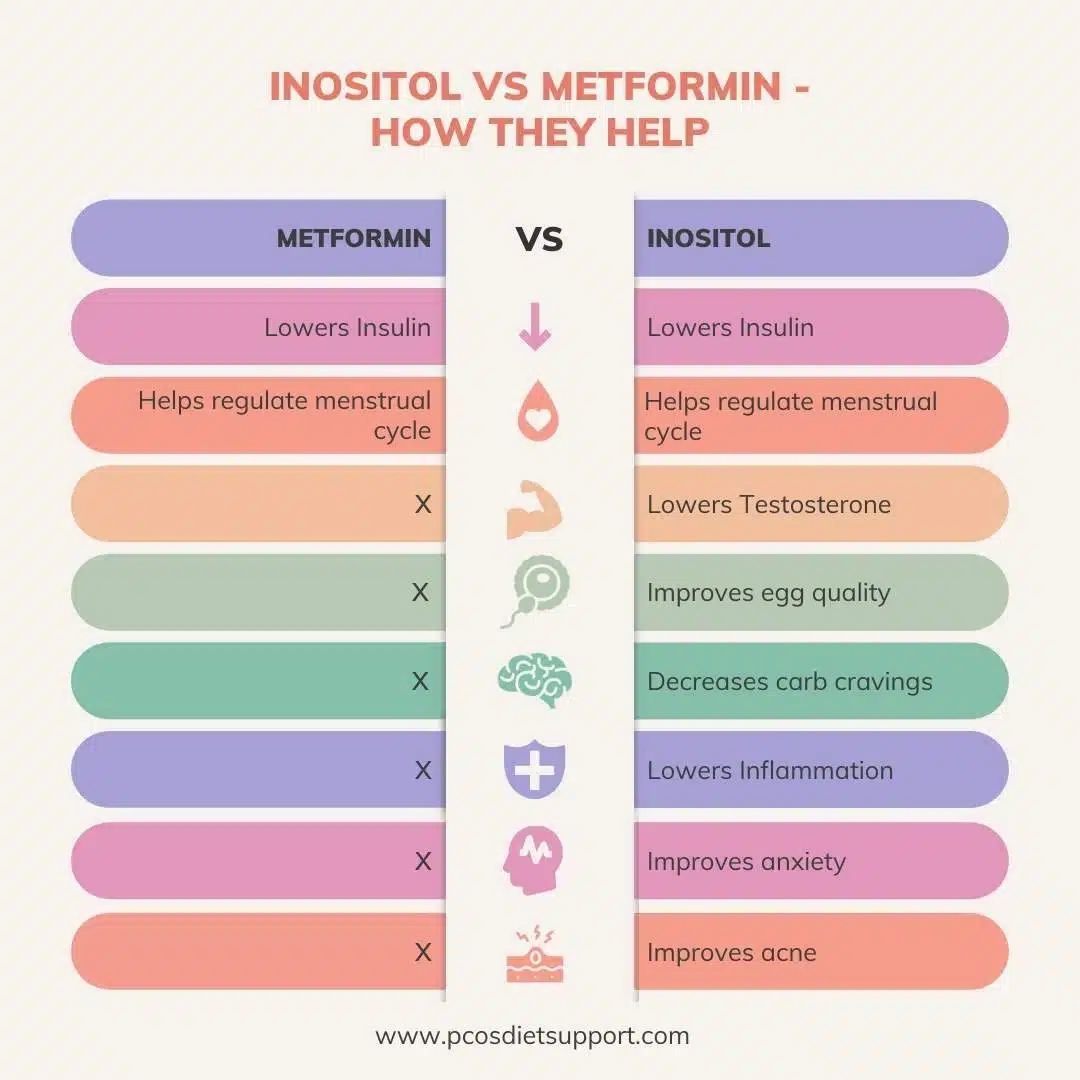
When evaluating these two options, clinicians look at several key metrics: androgen reduction, ovulation restoration, and the side-effect profile.
Data from randomized clinical trials suggest that Metformin is highly effective at reducing fasting blood sugar and improving the lipid profile. However, its drawbacks are significant. Approximately 30% to 50% of patients report gastrointestinal issues, including nausea, diarrhea, and abdominal cramping. Long-term use of Metformin has also been linked to Vitamin B12 deficiency, which can lead to fatigue and nerve damage if not addressed.
In contrast, Inositol is remarkably well-tolerated. Because it is a substance already present in the human diet and body, the incidence of side effects is low. Some users report mild headaches or digestive upset at very high doses, but these are typically transient. Furthermore, Inositol has shown a specific benefit that Metformin lacks: it improves the quality of the eggs produced by the ovaries. For women undergoing In-Vitro Fertilization (IVF) or trying to conceive naturally, this makes Inositol a particularly attractive option.

Supporting Data and Clinical Outcomes
A 2021 systematic review and meta-analysis analyzed the effects of Myo-inositol versus Metformin on ovarian function. The researchers concluded that there was no significant difference in the pregnancy rates between the two groups. However, the Myo-inositol group showed a significantly lower risk of adverse events.
Another study focusing on metabolic parameters found that while both treatments reduced testosterone levels, Metformin was slightly more effective at lowering fasting insulin, whereas Inositol was more effective at improving the FSH/LH (Follicle Stimulating Hormone to Luteinizing Hormone) ratio, which is a critical marker for reproductive health in PCOS.
Reactions from the Medical Community and Patients
The medical community’s response to the Inositol vs. Metformin debate has shifted toward a more patient-centric model. Endocrinologists often note that while Metformin is a powerful tool for those with significant insulin resistance or pre-diabetes, the "barrier to entry" is high due to the physical discomfort it causes.

Patient advocacy groups, such as those within the PCOS Foodies community, frequently report that Inositol provides a "gentler" path to management. Many women who were forced to discontinue Metformin due to severe nausea found success with Inositol, reporting regular cycles for the first time in years. However, medical professionals emphasize that Inositol is a supplement and not a regulated drug, meaning the quality of the product can vary significantly between brands.
Broader Impact and Future Implications
The ongoing comparison between these two agents highlights a growing trend toward "Precision Medicine" in women’s health. Rather than a one-size-fits-all prescription of birth control pills—which manage symptoms but do not address the underlying metabolic cause—doctors are increasingly looking at the metabolic "phenotype" of the patient.
For a patient with severe obesity and a high risk of progressing to Type 2 diabetes, Metformin remains a vital clinical tool. For a patient focused on fertility, egg quality, and minimizing side effects, Inositol appears to be the superior choice. There is also increasing interest in "combination therapy." Because Metformin and Inositol work on different parts of the insulin signaling pathway, some research suggests that taking both together in lower doses can provide a synergistic effect, maximizing metabolic benefits while minimizing the side effects of Metformin.
As the body of research grows, the consensus is leaning toward Inositol as a primary intervention for the average PCOS patient. Its safety profile, combined with its efficacy in restoring ovulation and improving egg quality, positions it as a cornerstone of modern PCOS management. Nevertheless, the transition from any medication to a supplement, or the combination of the two, should only be done under the strict supervision of a healthcare provider to monitor blood glucose levels and ensure the safety of the endocrine system.
The future of PCOS treatment lies in this nuanced understanding of metabolic health, where the choice between a lab-synthesized drug and a nature-derived supplement is determined by the specific physiological needs and life goals of the individual woman.
