
Polycystic Ovary Syndrome (PCOS) remains the most prevalent endocrine disorder among women of reproductive age globally, affecting an estimated 8% to 13% of the female population. Characterized by a combination of hyperandrogenism, ovulatory dysfunction, and polycystic ovarian morphology, the syndrome is increasingly recognized not merely as a reproductive issue but as a complex metabolic condition. Central to the pathophysiology of PCOS is insulin resistance, a state in which the body’s cells become less responsive to insulin, leading the pancreas to overproduce the hormone to maintain stable blood glucose levels. This hyperinsulinemia serves as a primary driver for many PCOS symptoms, prompting a long-standing clinical debate regarding the optimal choice of insulin-sensitizing agents: the pharmaceutical mainstay Metformin or the nutrient-based supplement Inositol.
The Physiological Foundation of Insulin Resistance in PCOS
Insulin resistance is estimated to affect up to 75% of women with PCOS, including those within a healthy weight range. When insulin levels remain chronically elevated, the hormone acts synergistically with luteinizing hormone (LH) to stimulate the theca cells within the ovaries. This stimulation results in the overproduction of androgens, such as testosterone. High androgen levels, in turn, interfere with follicular development, leading to irregular menstrual cycles, hirsutism, acne, and male-pattern hair loss.

Furthermore, excess insulin inhibits the production of Sex Hormone-Binding Globulin (SHBG) in the liver. SHBG is a protein that binds to testosterone in the blood; when SHBG levels are low, more "free" testosterone is available to affect the body’s tissues, exacerbating clinical symptoms. Because of this intricate link between insulin and reproductive hormones, clinical interventions have historically focused on improving insulin sensitivity as a foundational treatment for the syndrome.
Metformin: The Pharmaceutical Standard for Glycemic Control
Metformin, a biguanide class medication, has been a cornerstone in the treatment of Type 2 diabetes for decades. Although its use for PCOS is considered "off-label" in many jurisdictions, it is widely prescribed by endocrinologists and gynecologists to address the metabolic facets of the disorder.
Metformin functions through three primary mechanisms. First, it reduces the amount of glucose produced by the liver (gluconeogenesis). Second, it increases the sensitivity of muscle cells to insulin, allowing for more efficient glucose uptake. Third, it slows the absorption of carbohydrates in the intestinal tract. By lowering circulating glucose and insulin, Metformin indirectly reduces ovarian androgen production and can help restore regular ovulation.

Clinical data supporting Metformin is extensive. Research indicates that the medication can significantly improve pregnancy rates and reduce the risk of progressing to Type 2 diabetes in women with PCOS. However, despite its efficacy in hormonal and glycemic regulation, Metformin’s impact on Body Mass Index (BMI) remains inconsistent. While some patients experience modest weight loss, randomized controlled trials have shown that many women see little to no change in body weight after six months of therapy, suggesting that the drug’s primary value lies in metabolic signaling rather than weight reduction.
Inositol: A Nutrient-Based Approach to Cellular Signaling
Inositol, often referred to as Vitamin B8 (though technically a carbocyclic sugar), is a naturally occurring compound found in fruits, beans, grains, and nuts. In the context of PCOS, two specific isomers—Myo-inositol (MI) and D-chiro-inositol (DCI)—have gained significant attention. These molecules act as "second messengers" in the insulin signaling pathway.
When insulin binds to a cell receptor, inositol-containing molecules are required to transmit the signal into the cell to activate glucose transporters. In many women with PCOS, there appears to be a defect in this inositol-dependent signaling, contributing to insulin resistance. Myo-inositol, in particular, is vital for the activation of transporters that allow glucose to enter the cell and is also involved in the signaling of Follicle-Stimulating Hormone (FSH), which is essential for egg quality and ovulation.

Recent comparative studies have positioned Inositol as a formidable alternative to Metformin. A 2021 systematic review and meta-analysis published in the European Review for Medical and Pharmacological Sciences found that Myo-inositol was as effective as Metformin in improving insulin resistance, reducing androgen levels, and restoring regular menstrual cycles. Furthermore, Inositol has shown specific benefits for oocyte (egg) quality, making it a preferred option for many fertility specialists.
Clinical Chronology: The Shift Toward Integrative Management
The history of PCOS treatment has undergone a significant transformation over the last thirty years. In the 1990s, the discovery of the link between insulin and the ovaries led to the first widespread use of Metformin in PCOS populations. Throughout the early 2000s, Metformin was the primary non-hormonal intervention recommended for those seeking to restore fertility or manage metabolic risks.
However, the late 2000s and early 2010s saw a surge in research regarding the role of inositols. Initial studies focused on Myo-inositol’s ability to induce ovulation in women who were "Metformin-resistant." By 2018, the International Evidence-based Guideline for the Assessment and Management of Polycystic Ovary Syndrome acknowledged the potential of Inositol, though it noted that more large-scale trials were needed to achieve the same level of evidence as Metformin.

Today, the medical community is increasingly moving toward a personalized approach. The chronology of treatment often begins with lifestyle modifications—diet and exercise—followed by the introduction of an insulin sensitizer. The choice between Metformin and Inositol is now frequently dictated by the patient’s specific symptoms, fertility goals, and tolerance for side effects.
Comparative Efficacy: Analyzing Clinical Outcomes
When comparing the two agents side-by-side, researchers look at several key metrics: insulin sensitivity, androgen reduction, and reproductive outcomes.
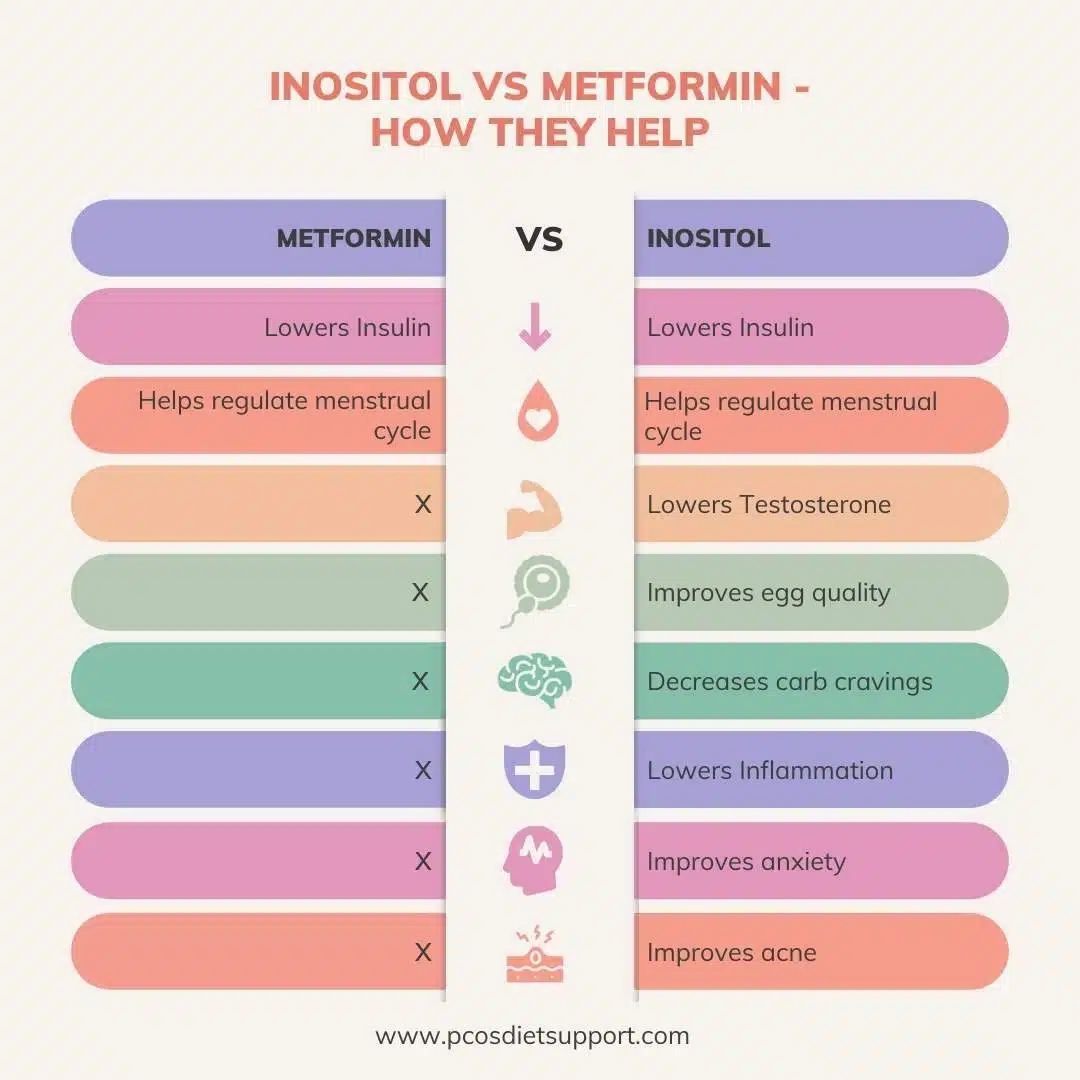
- Insulin Sensitivity: Both Metformin and Myo-inositol effectively lower HOMA-IR (Homeostatic Model Assessment for Insulin Resistance) scores. Metformin tends to have a more potent effect on fasting blood sugar levels, while Inositol is highly effective at managing the post-prandial (after-meal) insulin response.
- Hyperandrogenism: Both treatments contribute to lower testosterone levels and increased SHBG. This leads to improvements in acne and hirsutism, though these changes often take three to six months to become clinically visible.
- Ovulation and Fertility: Inositol has shown a slight edge in some studies regarding egg quality. Because Myo-inositol is involved in the FSH signaling pathway within the ovary, it may provide superior support for follicular maturation compared to Metformin, which primarily works on systemic insulin levels.
- Weight Management: Neither treatment is a "weight loss drug" in the traditional sense. However, by correcting the underlying insulin signaling, both can make it easier for patients to lose weight through diet and exercise. Some evidence suggests that Inositol may have a better impact on reducing the waist-to-hip ratio.
Side Effect Profiles and Long-Term Tolerability
The most significant divergence between Metformin and Inositol lies in their side effect profiles. Metformin is notorious for gastrointestinal distress. Between 20% and 50% of patients report side effects such as nausea, abdominal cramping, diarrhea, and a metallic taste in the mouth. These symptoms are often dose-dependent and can be so severe that patients discontinue the medication. Furthermore, long-term Metformin use has been linked to Vitamin B12 deficiency, necessitating regular monitoring and supplementation.

In contrast, Inositol is generally considered to be exceptionally well-tolerated. Because it is a compound naturally found in the human diet and produced by the body, the risk of adverse reactions is low. The most common side effects are mild digestive upset or headaches, which typically occur only at very high dosages. This high tolerability often leads to better patient compliance compared to Metformin.
Broader Implications for Reproductive and Metabolic Health
The debate between Inositol and Metformin reflects a broader shift in modern medicine toward "nutraceuticals"—supplements that provide medical or health benefits. For women with PCOS, the availability of a non-pharmaceutical option like Inositol offers a sense of autonomy and a reduction in the "medicalization" of their condition.
However, medical professionals caution against viewing Inositol as a complete replacement for Metformin in all cases. For women with significant metabolic derangement, pre-diabetes, or those who are at high risk for cardiovascular disease, Metformin’s potent effect on hepatic glucose production may be necessary. Some practitioners are now experimenting with combination therapy, using lower doses of both Metformin and Inositol to maximize benefits while minimizing the gastrointestinal side effects of the former.
From a public health perspective, the implications are significant. As PCOS is a precursor to Type 2 diabetes and metabolic syndrome, the effective use of insulin sensitizers can reduce the long-term burden on healthcare systems. Whether through the pharmaceutical path of Metformin or the supplemental path of Inositol, addressing the root cause of insulin resistance is essential for the long-term health of millions of women.
Conclusion and Future Directions
In conclusion, both Metformin and Inositol serve as effective tools in the management of PCOS, each with a unique mechanism of action and clinical profile. Metformin remains a powerful, evidence-backed pharmaceutical option for glycemic control, while Inositol offers a natural, highly tolerable alternative that may provide specific advantages for fertility and egg quality.
As research continues to evolve, the focus is likely to shift toward identifying specific biomarkers that can predict which patients will respond best to which treatment. For now, the consensus among experts suggests that the choice should be made through a shared decision-making process between the patient and their healthcare provider, taking into account metabolic needs, reproductive goals, and the individual’s tolerance for side effects. In the evolving landscape of PCOS care, the integration of both traditional medicine and targeted supplementation represents the most promising path forward for holistic symptom management.
