
Polycystic Ovary Syndrome (PCOS) remains the leading endocrine disorder among women of reproductive age globally, characterized by a complex interplay of hormonal imbalances, ovulatory dysfunction, and metabolic disturbances. Central to the pathophysiology of this condition is insulin resistance, a state where the body’s tissues become less responsive to insulin, leading to compensatory hyperinsulinemia. To address these systemic issues, healthcare providers have increasingly turned to insulin sensitizers. The two most prominent options in contemporary clinical practice are Metformin, a long-standing pharmaceutical intervention for Type 2 diabetes, and Inositol, a naturally occurring sugar alcohol that has gained significant traction as a therapeutic supplement. As the medical community seeks to optimize long-term management strategies for PCOS, a rigorous comparison of these two agents reveals distinct advantages, side-effect profiles, and mechanisms of action that influence patient adherence and clinical success.
The Physiological Imperative: Insulin Resistance in PCOS
Insulin resistance is not merely a comorbid condition of PCOS; it is a primary driver of the syndrome’s most distressing symptoms. Clinical data indicates that up to 75% of women diagnosed with PCOS exhibit some degree of impaired insulin sensitivity, regardless of their Body Mass Index (BMI). When the body produces excess insulin to compensate for resistance, the hormone acts synergistically with luteinizing hormone (LH) to stimulate the theca cells within the ovaries. This stimulation results in the overproduction of androgens, such as testosterone, which manifests clinically as acne, hirsutism (excess hair growth), and male-pattern hair loss.

Furthermore, hyperinsulinemia disrupts the delicate signaling required for regular ovulation. High insulin levels can inhibit the production of Sex Hormone-Binding Globulin (SHBG) in the liver, further increasing the amount of free, biologically active testosterone in the bloodstream. This hormonal cascade often leads to the formation of small, immature follicles on the ovaries—the "cysts" from which the syndrome derives its name—and results in irregular menstrual cycles or infertility. Consequently, the use of insulin sensitizers like Metformin and Inositol is designed to break this cycle by improving the body’s glucose metabolism and lowering systemic insulin levels.
Metformin: The Traditional Pharmaceutical Standard
Metformin has served as a cornerstone of metabolic medicine since its approval for Type 2 diabetes. While its use in PCOS is technically "off-label" in many jurisdictions, it is widely recognized by international guidelines as a secondary treatment for metabolic complications associated with the syndrome. Metformin belongs to the biguanide class of medications and functions primarily by activating the adenosine monophosphate-activated protein kinase (AMPK) pathway.
Medical researchers have identified three primary mechanisms through which Metformin assists PCOS patients. First, it suppresses hepatic gluconeogenesis, meaning it reduces the amount of glucose the liver releases into the bloodstream. Second, it enhances peripheral insulin sensitivity by increasing glucose uptake in the skeletal muscles. Third, it slows the absorption of glucose from the gastrointestinal tract. A landmark study published in the Journal of Clinical Endocrinology & Metabolism demonstrated that Metformin treatment significantly improved ovulation rates and reduced androgen levels in women with PCOS, particularly those with higher baseline insulin levels.

Despite its efficacy, Metformin is frequently associated with a high rate of discontinuation due to gastrointestinal side effects. Patients often report nausea, abdominal cramping, and diarrhea, particularly during the initiation phase of treatment. Furthermore, long-term Metformin use has been linked to a higher risk of Vitamin B12 deficiency, necessitating regular monitoring and supplementation to prevent neurological complications and anemia.
Inositol: The Emergence of Targeted Supplementation
Inositol, specifically in the forms of Myo-inositol (MI) and D-chiro-inositol (DCI), represents a newer frontier in PCOS management. Often referred to as Vitamin B8—though technically a carbocyclic sugar—inositol acts as a "second messenger" in insulin signaling. When insulin binds to its receptor on the cell wall, it triggers the release of inositol-containing molecules (inositoglycans) that carry the signal inside the cell to activate glucose transporters.
In women with PCOS, there is often a functional deficiency in these inositol messengers or an imbalance in the MI to DCI ratio. Myo-inositol is particularly crucial for egg quality and the follicle-stimulating hormone (FSH) signal, while D-chiro-inositol is involved in glucose storage and androgen synthesis. Clinical trials, including a systematic review and meta-analysis published in European Review for Medical and Pharmacological Sciences, have shown that Myo-inositol is as effective as Metformin in improving insulin sensitivity and reducing clinical androgenism, but with a significantly lower side-effect profile.

The mechanism of Inositol is inherently more "cellular" than Metformin’s systemic approach. By facilitating the "lock and key" mechanism of the insulin receptor, Inositol allows cells to process glucose more efficiently, thereby signaling the pancreas to reduce insulin production. This targeted action not only improves metabolic markers but has also shown superior results in improving oocyte (egg) quality in women undergoing Invitro Fertilization (IVF).
Comparative Clinical Analysis and Side-Effect Profiles
When comparing the two agents side-by-side, the clinical choice often hinges on the patient’s specific goals—whether they are seeking fertility, weight loss, or the management of dermatological symptoms—and their tolerance for medication.
Metabolic and Reproductive Efficacy
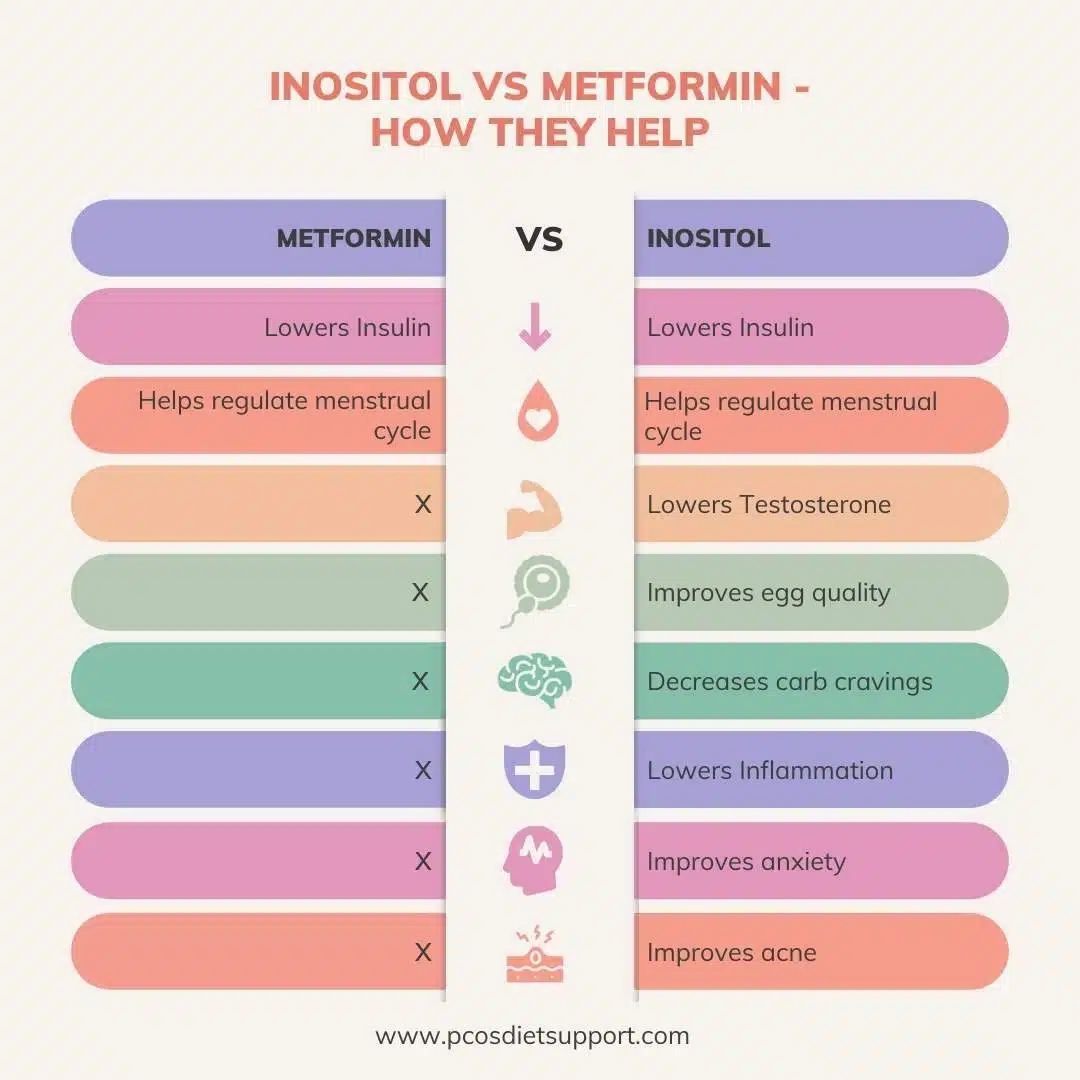
Research comparing the two indicates that both Metformin and Inositol are effective at restoring menstrual regularity and lowering testosterone. However, Inositol has shown a slight edge in reproductive outcomes. In a head-to-head study, women taking Myo-inositol reached their first ovulation faster than those on Metformin. Conversely, Metformin is often viewed as having a more robust effect on reducing fasting blood glucose and may be preferred for patients who are at an immediate risk of progressing to Type 2 diabetes.

Tolerability and Adherence
The most significant divergence between the two is found in patient experience. Metformin’s side effects are systemic and can be debilitating for some. Approximately 20% to 30% of patients experience significant gastrointestinal distress. In contrast, Inositol is generally considered very safe and well-tolerated. Because it is a substance naturally found in the human diet (in fruits, beans, and grains), the body processes supplemental inositol with minimal friction. Reported side effects for inositol are rare and usually limited to mild nausea or headaches at very high dosages.
Weight Management
While both treatments assist in the metabolic health required for weight loss, neither is a "weight loss drug" in the traditional sense. A study involving 120 women found that while Metformin led to a slightly higher reduction in BMI over six months compared to Inositol, the difference was not statistically significant enough to declare one superior for weight loss alone. Both require concurrent lifestyle and dietary interventions to be effective.
Chronology of Treatment Evolution
The shift in the medical landscape from Metformin to Inositol reflects a broader trend toward integrative and personalized medicine.

- 1990s – Early 2000s: Metformin becomes the primary "off-label" tool for PCOS following the realization that the condition was metabolic, not just gynecological.
- 2010 – 2015: Research into Myo-inositol gains momentum in Europe, particularly Italy, showing promising results for fertility.
- 2016 – 2020: Large-scale meta-analyses begin to confirm that Inositol is a viable alternative to Metformin, leading to the commercial popularity of supplements like Ovasitol (a 40:1 MI/DCI blend).
- Present Day: Clinical practice often involves a "patient-first" approach where Inositol is recommended as a first-line intervention for those wary of pharmaceutical side effects, while Metformin is reserved for more severe cases of insulin resistance or as a dual-therapy approach.
Official Responses and Expert Perspectives
The medical community remains cautious but optimistic regarding the integration of these treatments. The Endocrine Society and the International PCOS Network have updated their guidelines to acknowledge the role of insulin sensitizers, though they emphasize that lifestyle modification remains the "gold standard" first-line therapy.
Nutritional experts, such as Angela Grassi, RD, have noted that many patients find success in combining the two. Since Metformin and Inositol work on different parts of the insulin signaling pathway—Metformin on the AMPK pathway and Inositol on the secondary messenger system—they can theoretically act synergistically. However, practitioners warn that taking both simultaneously increases the risk of hypoglycemia (low blood sugar), and such a regimen must be strictly monitored by a physician.
Broader Implications for PCOS Management
The "Inositol vs. Metformin" debate highlights a critical evolution in how chronic endocrine disorders are managed. For decades, the pharmaceutical approach was the only option for women struggling with the metabolic fallout of PCOS. The rise of Inositol represents a shift toward using bio-identical substances to correct physiological deficiencies.
The implications of this shift are twofold. First, it empowers patients who may have previously abandoned treatment due to Metformin’s side effects to re-engage with their metabolic health. Second, it underscores the necessity for more rigorous regulation and standardization in the supplement industry to ensure that the inositol products patients consume are of the same purity and ratio used in clinical trials.
As research continues, the focus is shifting toward identifying which "phenotype" of PCOS patient responds best to which treatment. For the woman seeking to regulate her cycle with minimal disruption to her daily life, Inositol appears to be the burgeoning favorite. For the patient with severe insulin resistance and a family history of diabetes, Metformin remains a powerful and necessary tool. Ultimately, the choice between Inositol and Metformin is not a matter of which is "better" in a vacuum, but which is more appropriate for the individual patient’s metabolic profile and long-term health objectives.
