
Polycystic Ovary Syndrome (PCOS) remains the most prevalent endocrine disorder among women of reproductive age globally, affecting an estimated 8% to 13% of the population. Central to the pathology of this condition is insulin resistance, a metabolic state found in approximately 75% of diagnosed cases. To manage the myriad of symptoms associated with PCOS—ranging from irregular menstrual cycles and infertility to hirsutism and weight gain—clinicians frequently turn to insulin-sensitizing agents. For decades, Metformin has been the pharmaceutical standard, but the emergence of Myo-inositol as a potent nutritional supplement has sparked a significant clinical debate regarding which intervention offers the superior balance of efficacy and tolerability.
The Pathophysiological Foundation: Insulin Resistance in PCOS
To understand the utility of Metformin and Inositol, one must first examine the role of insulin in the female reproductive system. In a healthy metabolic state, insulin facilitates the uptake of glucose into cells for energy. However, in women with PCOS, the body’s cells often become less responsive to insulin. To compensate, the pancreas secretes higher levels of the hormone, leading to hyperinsulinemia.

Excessive insulin levels act directly and indirectly on the ovaries. High insulin levels stimulate the theca cells within the ovaries to produce excess androgens, such as testosterone. Furthermore, hyperinsulinemia reduces the liver’s production of sex hormone-binding globulin (SHBG), the protein responsible for binding and neutralizing testosterone in the bloodstream. The resulting "free" testosterone leads to the classic symptoms of PCOS: acne, hair loss on the scalp, and unwanted hair growth on the face and body. Perhaps most critically, this hormonal imbalance disrupts the maturation of follicles, leading to anovulation and infertility.
Metformin: The Clinical Standard for Metabolic Management
Metformin, a biguanide originally derived from the French lilac, has been the frontline treatment for Type 2 diabetes since the mid-20th century. Its application in PCOS began in the 1990s as researchers recognized the shared metabolic underpinnings of the two conditions.
Mechanisms of Action
Metformin addresses hyperinsulinemia through three primary pathways:

- Hepatic Glucose Production: It inhibits the liver’s ability to produce new glucose (gluconeogenesis), thereby reducing the baseline amount of sugar in the blood.
- Intestinal Absorption: It slows the absorption of glucose from the digestive tract into the bloodstream following meals.
- Insulin Sensitivity: It activates the enzyme AMPK, which increases the sensitivity of muscle and fat cells to existing insulin, allowing the body to process glucose more efficiently with less hormonal output.
Clinical Benefits and Research Data
Extensive longitudinal studies have validated Metformin’s role in managing PCOS. Research indicates that Metformin therapy can lead to a significant reduction in fasting blood sugar and a decrease in androgen levels. A landmark study published in The Journal of Clinical Endocrinology & Metabolism demonstrated that Metformin could restore regular ovulation in approximately 30% to 50% of women who were previously anovulatory. Furthermore, it is often prescribed to reduce the risk of developing gestational diabetes in women with PCOS who achieve pregnancy.
The Emergence of Inositol: A Nutrient-Based Alternative
While Metformin is a synthetic drug, Inositol is a naturally occurring sugar alcohol found in fruits, beans, and grains. Though often referred to as Vitamin B8, it is technically a carbohydrate that the human body can synthesize. In the context of PCOS, two specific isomers are of interest: Myo-inositol (MI) and D-chiro-inositol (DCI).
The Signaling Pathway
Inositol acts as a "second messenger" in insulin signaling. When insulin binds to a cell receptor, inositol-containing molecules (inositol phosphoglycans) are released to carry the signal into the cell, effectively "unlocking" the door for glucose. In many women with PCOS, there appears to be a defect in this signaling pathway or a deficiency in the inositol required to facilitate the process. Supplementation aims to bypass this defect, improving the "lock and key" mechanism of the insulin receptor.

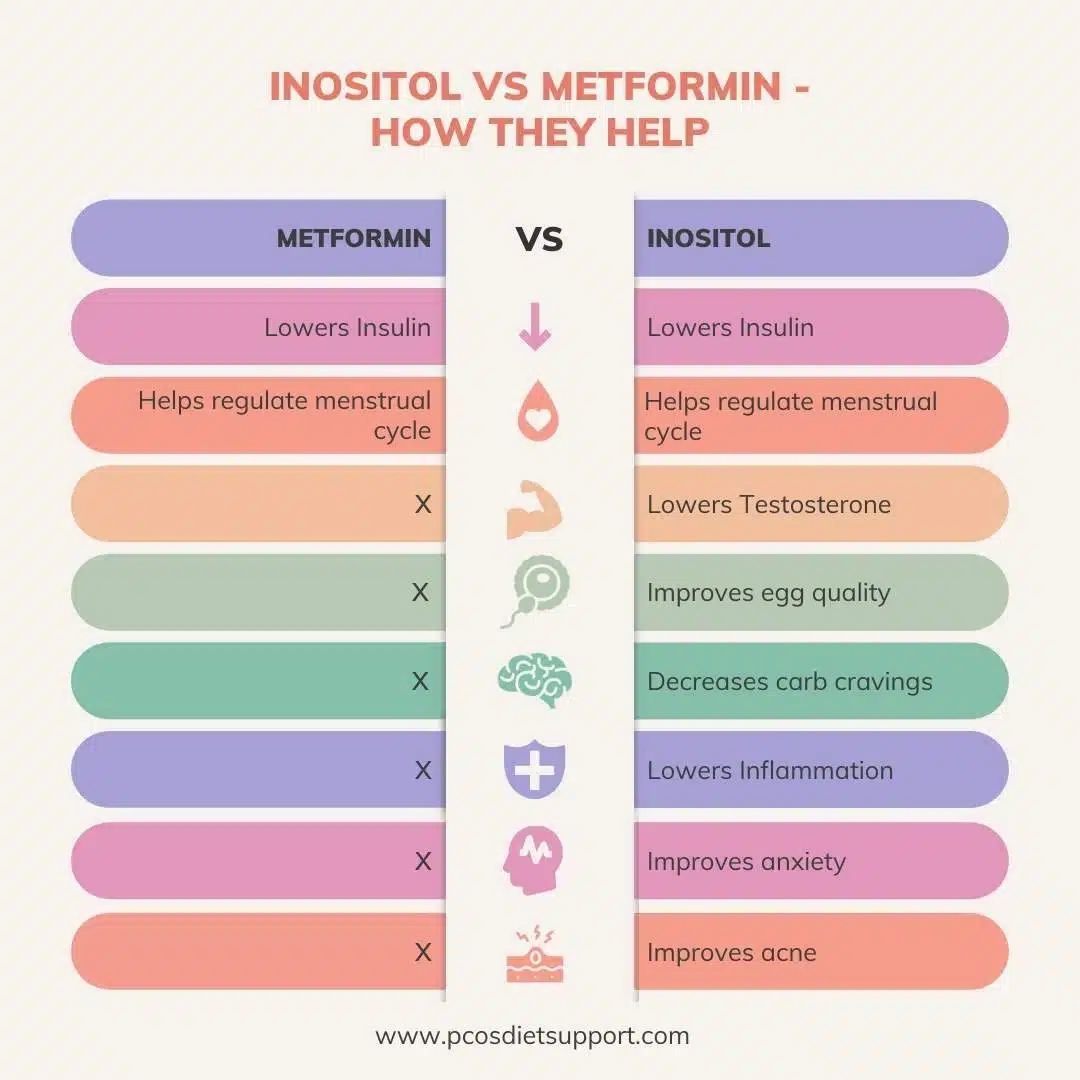
Clinical Efficacy Compared to Metformin
Recent meta-analyses have challenged the dominance of Metformin. A 2021 systematic review published in European Review for Medical and Pharmacological Sciences compared Myo-inositol and Metformin directly. The study concluded that Myo-inositol was essentially as effective as Metformin in improving insulin resistance, reducing androgen levels, and restoring regular menstrual cycles. Crucially, Myo-inositol was found to be superior in improving egg quality and reducing the risk of ovarian hyperstimulation syndrome (OHSS) during fertility treatments.
A Chronological Overview of Treatment Evolution
The shift from purely hormonal treatments to insulin-sensitizing approaches has evolved over the last century:
- 1922: Metformin is first synthesized, though its primary use remains obscure for decades.
- 1957: Metformin is approved in Europe for the treatment of diabetes.
- 1994: The first major clinical trials suggest Metformin can restore ovulation in women with PCOS.
- 1999: Research begins to emerge regarding the role of Inositol phosphoglycans in insulin signaling defects in PCOS patients.
- 2013-2018: A surge in randomized controlled trials compares Inositol isomers (Myo and D-chiro) against Metformin, establishing Inositol as a viable first-line alternative.
- 2023: International Evidence-based Guidelines for PCOS recognize Inositol as an experimental but increasingly supported therapy, particularly for those who cannot tolerate Metformin.
Comparative Side-Effect Profiles
The most significant divergence between the two treatments lies in patient tolerability. This factor often dictates long-term compliance and clinical success.

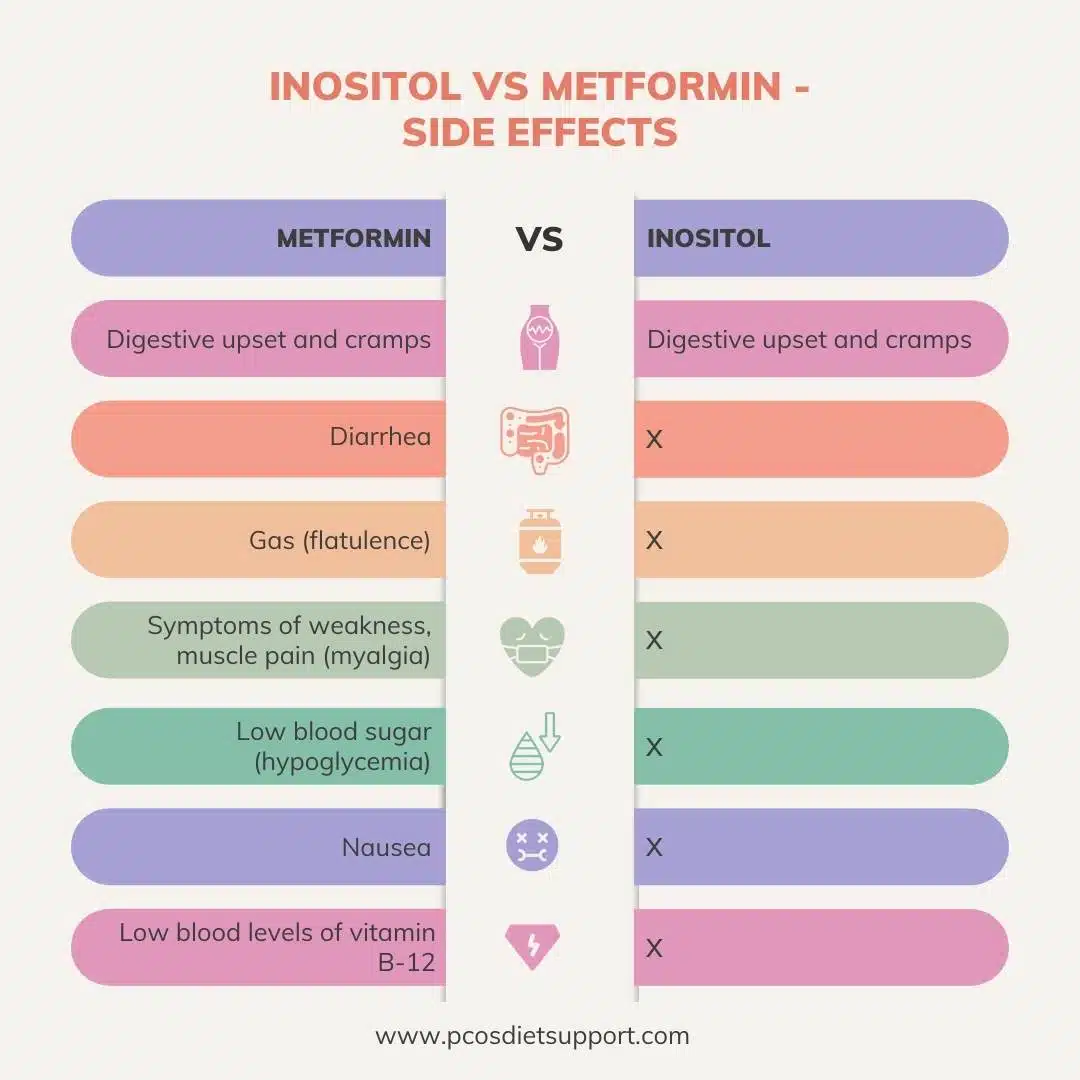
The Metformin Burden
Despite its efficacy, Metformin is notorious for gastrointestinal side effects. Clinical data suggests that up to 25% of patients experience:
- Nausea and vomiting.
- Severe abdominal cramping.
- Diarrhea.
- A metallic taste in the mouth.
Furthermore, long-term Metformin use is associated with a risk of Vitamin B12 deficiency. Because B12 is essential for nerve health and energy metabolism, patients on long-term therapy are generally advised to undergo annual screenings for deficiency.
The Inositol Advantage
In contrast, Myo-inositol is remarkably well-tolerated. Because it is a substance the body recognizes as a nutrient, side effects are rare. At very high doses (exceeding 12 grams per day), some patients report mild nausea or flatulence, but at the standard clinical dose of 4 grams per day, adverse effects are negligible. This high safety profile makes it an attractive option for women who have failed to maintain a Metformin regimen due to physical discomfort.

Weight Loss and Metabolic Markers: The Data
A common goal for PCOS patients is weight management. The data here is nuanced. While Metformin is often touted as a weight-loss drug, clinical trials show that its impact on Body Mass Index (BMI) is modest, often resulting in a loss of only 1-2 kilograms more than a placebo over six months.
Inositol shows similar results. While it improves the metabolic "environment"—lowering triglycerides and improving the LDL/HDL cholesterol ratio—neither Metformin nor Inositol acts as a primary weight-loss agent in the absence of dietary and lifestyle interventions. However, by stabilizing insulin, both treatments help reduce the intense sugar cravings that often sabotage weight-loss efforts in PCOS patients.
Synergistic Potential: Can They Be Taken Together?
Given that Metformin and Inositol work on different parts of the insulin pathway—Metformin primarily on the liver and gut, and Inositol on the cellular receptor signaling—some clinicians have begun exploring combination therapy.
Preliminary studies suggest that taking both may yield better results for insulin sensitivity than taking either alone. However, this approach requires strict medical supervision. Because both are insulin sensitizers, the combination increases the risk of hypoglycemia (low blood sugar), which can cause dizziness, shakiness, and fainting. Furthermore, the combination does not alleviate the gastrointestinal issues associated with Metformin; in some cases, it may exacerbate them.
Broader Impact and Future Implications
The debate between Inositol and Metformin represents a broader shift in reproductive medicine toward "functional" and "nutraceutical" interventions. As the medical community moves toward personalized medicine, the choice between these two agents often comes down to the individual patient’s phenotype and goals.
For a patient with severe insulin resistance and a high risk of progressing to Type 2 diabetes, Metformin’s long-term safety data and potent glucose-lowering effects may make it the preferred choice despite the side effects. Conversely, for a patient focused on fertility, egg quality, and minimizing systemic side effects, Myo-inositol presents a compelling, evidence-based alternative.
The implications for public health are significant. With PCOS serving as a precursor to metabolic syndrome, cardiovascular disease, and endometrial cancer, providing effective and tolerable insulin-sensitizing options is a priority. As further research clarifies the optimal ratios of inositol isomers and the long-term impacts of combination therapies, the management of PCOS is expected to become increasingly refined, moving away from a one-size-fits-all pharmaceutical approach toward a more integrated metabolic strategy.
In conclusion, while Metformin remains a powerful tool in the clinician’s arsenal with decades of supporting data, Myo-inositol has proven itself to be a formidable peer. The lack of significant side effects associated with Inositol, combined with its comparable efficacy in restoring hormonal balance and ovulation, positions it as a leading choice for the modern management of Polycystic Ovary Syndrome. Patients are advised to consult with healthcare providers to determine which path aligns best with their specific metabolic profile and reproductive objectives.
