
Polycystic Ovary Syndrome (PCOS) remains the most prevalent endocrine disorder among women of reproductive age globally, affecting an estimated 8% to 13% of the population. As medical understanding of the condition has evolved from a purely gynecological concern to a complex metabolic syndrome, the focus of treatment has shifted toward addressing insulin resistance. Among the most debated interventions in contemporary clinical practice is the comparative efficacy of Metformin, a long-standing pharmaceutical staple for type 2 diabetes, and Inositol, a naturally occurring sugar alcohol that has gained significant traction as a therapeutic supplement. Both agents function as insulin sensitizers, yet they possess distinct mechanisms, side-effect profiles, and clinical outcomes that necessitate a detailed examination for patients and healthcare providers alike.
The Metabolic Foundation: Insulin Resistance in PCOS
To understand the utility of insulin sensitizers, it is essential to establish the physiological context of PCOS. Clinical research indicates that upwards of 75% of women diagnosed with the condition exhibit some degree of insulin resistance, regardless of their Body Mass Index (BMI). In these cases, the body’s cells become less responsive to insulin, the hormone responsible for regulating blood glucose. Consequently, the pancreas compensates by secreting higher levels of insulin, leading to hyperinsulinemia.

This excess insulin acts as a primary driver for the symptomatic manifestations of PCOS. It stimulates the ovarian theca cells to produce excessive amounts of androgens, such as testosterone, which results in hirsutism, acne, and male-pattern hair loss. Furthermore, high insulin levels disrupt the delicate balance of the hypothalamic-pituitary-ovarian axis, often halting ovulation and leading to irregular menstrual cycles or infertility. By improving insulin sensitivity, interventions like Metformin and Inositol aim to lower circulating insulin levels, thereby addressing the root cause of these hormonal imbalances.
Metformin: The Clinical Standard for Metabolic Management
Metformin, a biguanide derivative, has been the "gold standard" for managing glucose levels in type 2 diabetes since its approval by the FDA in the mid-1990s. While its use for PCOS remains "off-label" in many jurisdictions, it is widely prescribed by endocrinologists and gynecologists due to its robust clinical history.
The pharmaceutical action of Metformin is threefold. First, it suppresses hepatic glucose production, meaning it reduces the amount of sugar the liver releases into the bloodstream. Second, it increases the sensitivity of muscle cells to insulin, enhancing peripheral glucose uptake and utilization. Third, it delays intestinal glucose absorption. Beyond glucose management, Metformin has been shown to increase levels of Sex Hormone-Binding Globulin (SHBG), a protein that binds to testosterone in the blood, effectively reducing the amount of "free" testosterone available to cause androgenic symptoms.

A landmark study published in the journal Human Reproduction highlighted that Metformin significantly improves ovulation rates and clinical pregnancy rates in women with PCOS. However, the study also noted that while Metformin is effective for metabolic parameters, its impact on weight loss is often modest and varies significantly between individuals.
Inositol: The Emerging Nutritional Powerhouse
Inositol, often referred to as Vitamin B8 (though technically a carbocyclic sugar), is found naturally in fruits, beans, grains, and nuts. In the context of PCOS, two specific isomers—Myo-inositol (MI) and D-chiro-inositol (DCI)—are of particular importance. These molecules serve as "second messengers" in the insulin signaling pathway.
The mechanism of Inositol is inherently biological. It acts at the cellular level to improve the "lock and key" mechanism of the insulin receptor. When insulin binds to a cell, inositol-containing phosphoglycans are released to signal the cell to open its glucose transporters. In many women with PCOS, there is a deficiency in these inositol messengers or an imbalance in the MI to DCI ratio, leading to a "signal failure" that results in insulin resistance. Supplementing with Inositol helps restore this signaling pathway, allowing the body to process glucose with less insulin.

Research, including a comprehensive meta-analysis published in the European Review for Medical and Pharmacological Sciences, suggests that Myo-inositol is as effective as Metformin in improving insulin sensitivity and reducing androgen levels. Furthermore, Inositol has shown specific promise in improving oocyte (egg) quality, which is a critical factor for women undergoing fertility treatments or struggling with miscarriage.
Comparative Efficacy and Clinical Data
When placed in a head-to-head comparison, the clinical data suggests a high degree of parity between the two treatments regarding their primary goals. A 2021 systematic review and meta-analysis evaluated the effects of Myo-inositol versus Metformin on ovarian function. The findings indicated no statistically significant difference between the two in terms of reducing the Ferriman-Gallwey score (a measure of excess hair growth) or improving pregnancy rates. Both interventions successfully lowered fasting insulin and reduced the Free Androgen Index.
However, a nuance emerges in the timeline of results. Metformin often shows a more rapid impact on blood glucose stabilization, whereas Inositol may require three to six months of consistent supplementation to achieve peak hormonal and ovulatory benefits. Conversely, Inositol has demonstrated a superior ability to restore regular menstrual cycles in some cohorts, particularly in younger women or those with a lower BMI who may not respond as traditionally to Metformin.

Patient Compliance and the Side-Effect Profile
The most significant divergence between Metformin and Inositol lies in patient tolerability. Metformin is notorious for its gastrointestinal side effects. Clinical data suggests that up to 30% of patients experience nausea, abdominal cramping, bloating, and diarrhea, particularly during the initial weeks of treatment. These symptoms can be severe enough to lead to high discontinuation rates. Furthermore, long-term Metformin use has been linked to Vitamin B12 deficiency, necessitating regular monitoring and supplementation.
In contrast, Inositol is generally considered to be exceptionally well-tolerated. Because it is a substance the body recognizes and produces naturally, side effects are rare. When they do occur, they are typically limited to mild digestive upset at very high doses. This high safety profile makes Inositol an attractive option for women who are sensitive to pharmaceutical side effects or those looking for a "natural" approach to symptom management.
Chronology of Treatment Evolution in PCOS
The approach to treating PCOS has undergone a significant transformation over the last three decades:

- 1990s: Treatment focused primarily on symptom suppression, using oral contraceptives to regulate periods and anti-androgens like Spironolactone to treat acne and hirsutism.
- Early 2000s: The link between PCOS and insulin resistance became widely accepted. Metformin moved from the world of diabetes into the gynecological toolkit, marking a shift toward metabolic treatment.
- 2010s: The "Inositol Revolution" began as researchers in Italy and elsewhere published breakthrough studies on Myo-inositol. Supplements like Ovasitol (a 40:1 MI to DCI ratio) entered the market, backed by clinical evidence.
- 2020s-Present: The current medical consensus is moving toward integrative medicine. Clinicians now frequently discuss "personalizing" the choice between Metformin and Inositol based on the patient’s specific phenotype, side-effect tolerance, and fertility goals.
Broader Impact and Implications for Long-term Health
The choice between Inositol and Metformin extends beyond immediate symptom relief; it has long-term implications for the prevention of secondary health complications. Women with PCOS are at a significantly higher risk for developing type 2 diabetes, cardiovascular disease, and endometrial cancer later in life.
By effectively managing insulin levels during the reproductive years, both Metformin and Inositol act as preventative measures. Metformin has a slight advantage in the clinical literature regarding long-term cardiovascular protection and weight management in obese patients. However, Inositol’s role in preventing gestational diabetes—a common complication for pregnant women with PCOS—is currently a burgeoning area of research, with early studies suggesting it may be more effective than Metformin in certain prenatal contexts.
Official Responses and Expert Perspectives
The international medical community has begun to formalize the role of these agents. The International PCOS Network, in its evidence-based guidelines, acknowledges Metformin as a recommended treatment for metabolic features and as an adjunct for fertility. While Inositol was previously categorized as "experimental," the sheer volume of recent positive data has led many experts, including recognized registered dietitians like Angela Grassi, to advocate for its use as a first-line therapy, particularly for those who cannot tolerate Metformin.
Medical professionals emphasize that these treatments are not mutually exclusive. In some clinical scenarios, doctors may prescribe a combination of both Metformin and Inositol. Because they work on different parts of the insulin signaling pathway, they can have a synergistic effect. However, patients are cautioned that combining two insulin sensitizers increases the risk of hypoglycemia (low blood sugar), and such a regimen should only be undertaken under strict medical supervision.
Summary of Findings
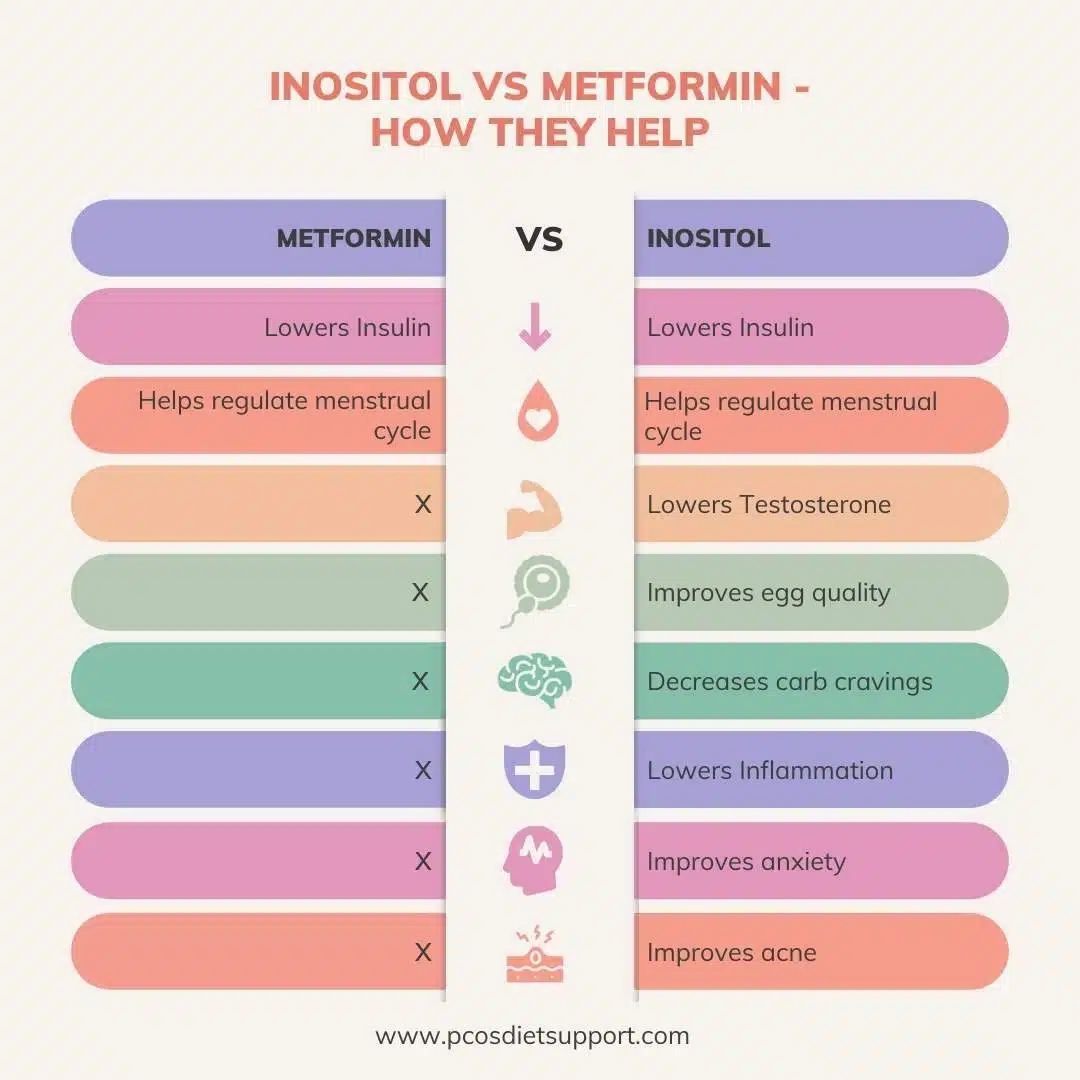
In the debate of Inositol versus Metformin, the "better" option is largely dependent on the individual patient’s priorities. Metformin offers a powerful, well-documented pharmaceutical intervention with secondary benefits for weight and long-term metabolic health, though it carries a high risk of gastrointestinal discomfort. Inositol provides a comparable level of efficacy for hormonal balance and ovulation with a near-zero side-effect profile, making it the preferred choice for those prioritizing tolerability and natural supplementation.
As the medical field continues to embrace a more nuanced understanding of PCOS, the dual availability of these agents provides a vital "safety net" for women. Whether through the calculated precision of Metformin or the biological harmony of Inositol, the goal remains the same: restoring metabolic balance to empower women to manage their symptoms and improve their overall quality of life. Patients are encouraged to consult with their healthcare providers to determine which insulin sensitizer aligns best with their unique physiological needs and long-term health objectives.
