
Polycystic Ovary Syndrome (PCOS) remains the most prevalent endocrine disorder among women of reproductive age globally, characterized by a complex interplay of hormonal imbalances, ovulatory dysfunction, and metabolic disturbances. Central to the pathophysiology of PCOS is insulin resistance, a condition affecting approximately 75% of diagnosed individuals, regardless of body mass index. As the medical community seeks more effective long-term management strategies, the debate between the use of Metformin, a long-standing pharmaceutical intervention, and Inositol, a naturally occurring nutrient-based supplement, has moved to the forefront of clinical discussion. Both substances function as insulin sensitizers, yet they offer distinct mechanisms of action, side effect profiles, and efficacy outcomes that necessitate a detailed comparative analysis.
The Pathophysiology of Insulin Resistance in PCOS
To understand the comparative utility of Metformin and Inositol, it is essential to examine the role of insulin in the female reproductive system. In a healthy metabolic state, insulin facilitates the uptake of glucose into cells for energy. However, in women with PCOS, cells often exhibit a diminished response to insulin signals. To compensate, the pancreas secretes higher levels of insulin (hyperinsulinemia) to maintain stable blood sugar levels.

This excess insulin acts as a co-gonadotropin, stimulating the ovarian theca cells to produce excessive amounts of androgens, such as testosterone. High androgen levels interfere with follicular development, leading to the "cysts" (undeveloped follicles) characteristic of the syndrome and resulting in symptoms such as hirsutism, acne, and irregular menstrual cycles. Furthermore, hyperinsulinemia inhibits the production of Sex Hormone Binding Globulin (SHBG) in the liver, further increasing the amount of free, active testosterone in the bloodstream. Consequently, any intervention that improves insulin sensitivity serves as a foundational treatment for the systemic symptoms of PCOS.
Metformin: The Pharmaceutical Standard
Metformin, a biguanide originally derived from the French lilac plant (Galega officinalis), has been the gold standard for treating Type 2 diabetes for decades. Although not specifically FDA-approved for PCOS, it is widely prescribed "off-label" to manage the metabolic and reproductive complications of the disorder.
Mechanisms of Action
Metformin targets insulin resistance through three primary pathways:

- Hepatic Glucose Inhibition: It reduces the amount of glucose produced by the liver (gluconeogenesis).
- Intestinal Absorption: It slows the absorption of carbohydrates in the digestive tract, preventing sharp spikes in post-prandial blood sugar.
- Peripheral Sensitivity: It enhances the sensitivity of muscle cells to insulin, allowing for more efficient glucose uptake.
Clinical Benefits and Data
Research, including a landmark study published in the Journal of Clinical Endocrinology & Metabolism, indicates that Metformin can significantly lower androgen levels and restore regular ovulation in approximately 30% to 50% of women with PCOS. By lowering circulating insulin, Metformin helps break the cycle of androgen overproduction. Furthermore, it has been associated with a reduction in the risk of developing gestational diabetes and may assist in modest weight loss for some patients, although weight loss is not a guaranteed outcome for all users.
Inositol: The Emerging Nutraceutical Alternative
Inositol is a carbocyclic sugar found in high concentrations in citrus fruits, beans, and grains. While often referred to as Vitamin B8, it is technically a sugar alcohol that the human body can synthesize from glucose. In the context of PCOS, two specific isomers are of clinical interest: Myo-inositol (MI) and D-chiro-inositol (DCI).
Mechanisms of Action
Inositol functions differently than Metformin. It acts as a "second messenger" in the insulin signaling pathway. When insulin binds to a cell receptor, inositol-containing molecules (inositoglycans) are released to trigger the internal cellular response. In women with PCOS, there is often a defect in this signaling mechanism or an imbalance in the ratio of MI to DCI.

- Myo-inositol: Primarily responsible for glucose uptake and the FSH (Follicle Stimulating Hormone) signaling at the ovarian level.
- D-chiro-inositol: Involved in glycogen synthesis and the reduction of androgen production.
Clinical Benefits and Data
A systematic review and meta-analysis published in the European Review for Medical and Pharmacological Sciences compared the effects of Myo-inositol and Metformin. The findings suggested that Myo-inositol is as effective as Metformin in improving insulin sensitivity, reducing clinical pregnancy rates, and lowering androgens. Notably, the study highlighted that Inositol appeared to have a superior effect on the maturation of oocytes (eggs), which is critical for women undergoing fertility treatments.
Comparative Chronology of Clinical Adoption
The integration of these treatments into standard PCOS protocols has followed a distinct timeline:
- 1990s: Metformin begins to see widespread off-label use for PCOS following studies highlighting the link between insulin and hyperandrogenism.
- Early 2000s: Research into Inositol isomers begins to emerge from Italy, suggesting that nutritional deficiencies in inositol might drive ovarian dysfunction.
- 2010-2015: Multiple randomized controlled trials (RCTs) establish that a 40:1 ratio of Myo-inositol to D-chiro-inositol (the physiological ratio found in plasma) provides the most optimal results for metabolic and reproductive health.
- 2018-Present: International evidence-based guidelines for PCOS acknowledge the role of Metformin for metabolic health but also recognize Inositol as an experimental yet promising therapy with a high safety profile.
Side Effect Profiles and Patient Compliance
One of the most significant factors in the Metformin vs. Inositol debate is tolerability. Patient compliance is often the deciding factor in the success of a long-term treatment plan.

Metformin Challenges
Metformin is notorious for gastrointestinal side effects. Clinical data suggests that up to 30% of patients experience nausea, abdominal cramping, and diarrhea, particularly during the initiation phase. Furthermore, long-term use of Metformin has been linked to Vitamin B12 deficiency, necessitating regular monitoring and supplementation. In rare cases, particularly in patients with renal impairment, it can lead to lactic acidosis, a serious medical condition.
Inositol Advantages
In contrast, Inositol is remarkably well-tolerated. Because it is a substance naturally found in the diet and produced by the body, side effects are rare and generally mild, typically limited to slight nausea or headaches at very high dosages. This high safety profile makes it an attractive option for women who cannot tolerate the therapeutic doses of Metformin required to see clinical improvements in PCOS symptoms.
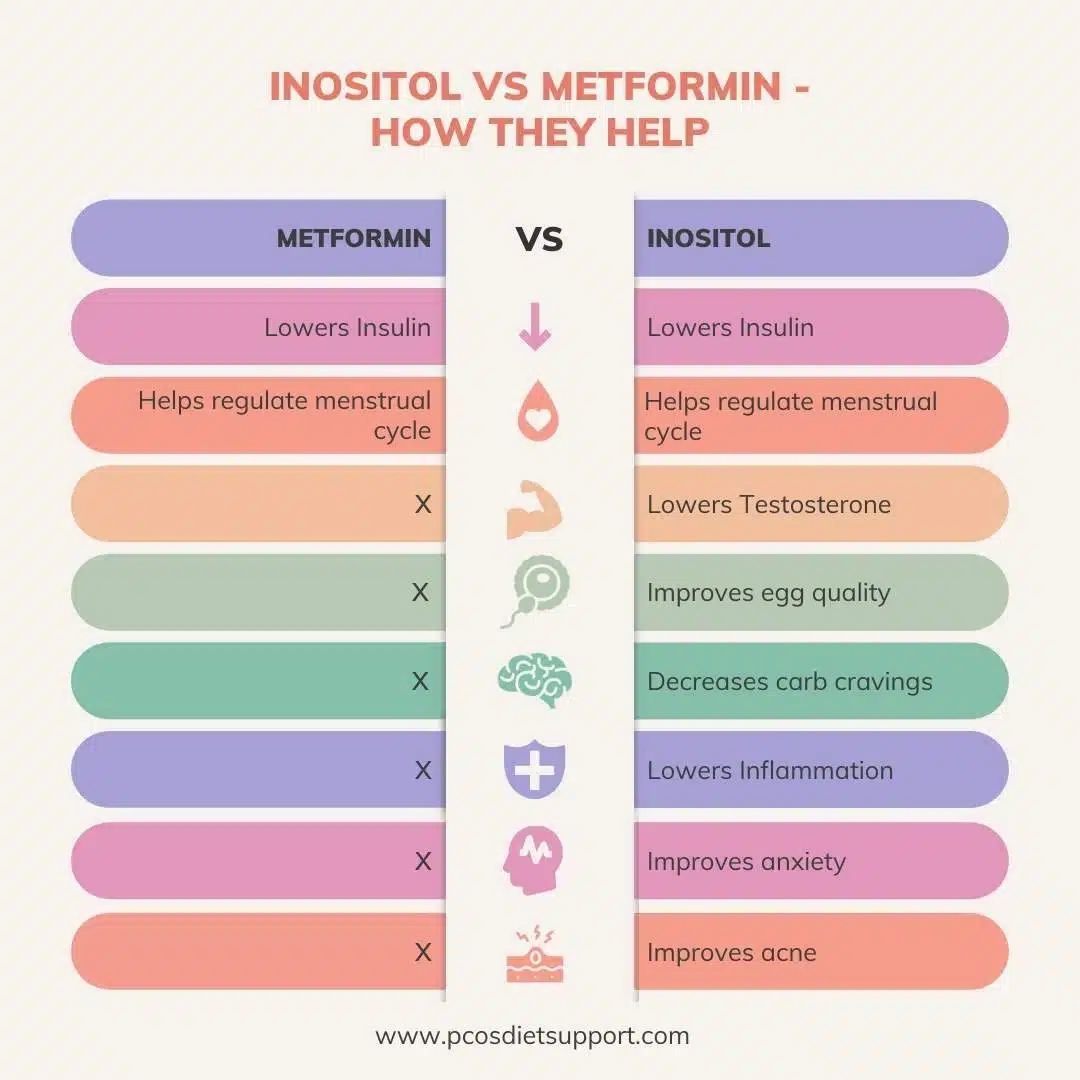
Side-by-Side Efficacy Comparison
| Feature | Metformin | Myo-Inositol |
|---|---|---|
| Primary Use | Pharmaceutical for Type 2 Diabetes | Nutritional Supplement |
| Insulin Sensitivity | High improvement | High improvement |
| Androgen Reduction | Significant | Significant |
| Ovulation Restoration | Effective | Effective (Potentially superior for egg quality) |
| Common Side Effects | Diarrhea, Nausea, Cramping | Minimal (Mild GI upset in rare cases) |
| Nutrient Impact | May cause Vitamin B12 deficiency | No known nutrient depletion |
| Availability | Prescription only | Over-the-counter |
Combined Therapy and Strategic Implications
Recent clinical inquiries have explored whether combining Metformin and Inositol provides a synergistic effect. Since they target insulin resistance through different biological pathways—Metformin by inhibiting hepatic glucose and Inositol by improving cellular signaling—some practitioners prescribe both simultaneously.

However, medical professionals caution that such a combination increases the risk of hypoglycemia (low blood sugar). "The dual-action approach can be highly effective for resistant cases," notes a summary of recent metabolic research, "but it requires careful titration and monitoring by a healthcare provider."
Broader Impact and Future Outlook
The shift toward Inositol represents a broader trend in endocrinology toward "metabolic flexibility" and the use of targeted nutraceuticals. While Metformin remains a powerful tool, especially for patients with significant weight issues or those at high risk for Type 2 diabetes, Inositol offers a gentler alternative for those focused primarily on fertility and cycle regulation.
The implications for the future of PCOS management are significant. As genomic testing becomes more accessible, doctors may soon be able to identify which patients have specific defects in the inositol signaling pathway versus those whose insulin resistance is driven primarily by hepatic factors. This would allow for a personalized medicine approach, where the choice between Metformin and Inositol is dictated by a patient’s unique molecular profile rather than trial and error.
In conclusion, both Metformin and Inositol are potent allies in the management of Polycystic Ovary Syndrome. Metformin carries the weight of decades of clinical validation but is hampered by a difficult side effect profile. Inositol offers a comparable level of efficacy for many PCOS symptoms with a significantly lower risk of adverse effects. Patients are encouraged to consult with endocrinologists or specialized reproductive health providers to determine which insulin sensitizer aligns best with their specific metabolic needs, fertility goals, and lifestyle preferences. As research continues to evolve, the integration of both pharmaceutical and nutritional strategies remains the most robust path forward for the millions of women navigating the complexities of PCOS.
