
Polycystic Ovary Syndrome (PCOS) remains the leading endocrine disorder among women of reproductive age globally, affecting an estimated 8% to 13% of the female population according to the World Health Organization. While traditionally viewed through the lens of reproductive health, modern clinical consensus has shifted to recognize PCOS as a complex metabolic condition deeply rooted in insulin resistance. As medical professionals and patients seek to manage the multifaceted symptoms of the syndrome—ranging from infertility and irregular cycles to hirsutism and weight gain—the debate between pharmaceutical intervention via Metformin and nutritional supplementation via Inositol has moved to the forefront of metabolic therapy.
The Pathophysiology of Insulin Resistance in PCOS
To understand the comparative utility of Metformin and Inositol, it is necessary to examine the role of insulin in the female endocrine system. Research indicates that up to 75% of lean women and 95% of women with a higher Body Mass Index (BMI) who have PCOS exhibit some degree of insulin resistance. In these individuals, the body’s peripheral tissues, such as muscle and fat, become less responsive to insulin. To compensate, the pancreas secretes higher levels of the hormone, leading to hyperinsulinemia.

Excessive insulin levels act as a co-gonadotropin, stimulating the ovarian theca cells to produce an overabundance of androgens, specifically testosterone. Furthermore, high insulin levels suppress the production of Sex Hormone-Binding Globulin (SHBG) in the liver, which normally binds to testosterone and renders it inactive. The resulting "free" testosterone is responsible for the clinical manifestations of PCOS, including acne, male-pattern hair loss (alopecia), and excessive body hair (hirsutism). Furthermore, hyperinsulinemia disrupts the delicate signaling required for follicular development, often leading to anovulation and subsequent infertility.
A Chronological Overview of PCOS Management
The treatment of PCOS has evolved significantly over the last four decades. In the 1980s and early 1990s, the focus was primarily on symptom management through oral contraceptives and anti-androgens. However, the mid-1990s marked a pivotal shift when researchers began to link the syndrome to Type 2 diabetes and cardiovascular risk.
In 1994, the first significant trials involving Metformin for PCOS began to emerge. Originally approved by the FDA in 1995 for Type 2 diabetes, Metformin became an "off-label" staple for PCOS management due to its ability to lower glucose production in the liver and increase peripheral insulin sensitivity. By the early 2000s, it was the gold-standard secondary treatment for women who did not respond to lifestyle changes.

The emergence of Inositol as a serious contender began in the late 2000s and early 2010s. Though Inositol was identified as a vital component in insulin signaling as early as the 1980s, it wasn’t until a series of landmark studies in Italy that the specific "Myo-inositol" and "D-chiro-inositol" isomers were recognized for their ability to restore ovulation and improve metabolic markers in PCOS patients with fewer side effects than traditional pharmaceuticals.
Metformin: The Pharmaceutical Mechanism and Clinical Data
Metformin is a biguanide antihyperglycemic agent. Its primary function is to inhibit gluconeogenesis—the process by which the liver produces glucose—thereby lowering the amount of sugar entering the bloodstream. Additionally, it activates adenosine monophosphate-activated protein kinase (AMPK), an enzyme that plays a crucial role in cellular energy homeostasis, effectively making the body’s cells more "hungry" for glucose and more sensitive to the insulin already present.
Clinical trials have consistently demonstrated Metformin’s efficacy. A meta-analysis of randomized controlled trials shows that Metformin significantly reduces fasting insulin levels and androgen levels in women with PCOS. It has also been shown to improve the regularity of menstrual cycles and, in some cases, assist with modest weight loss, although weight loss is not a guaranteed outcome for all patients.

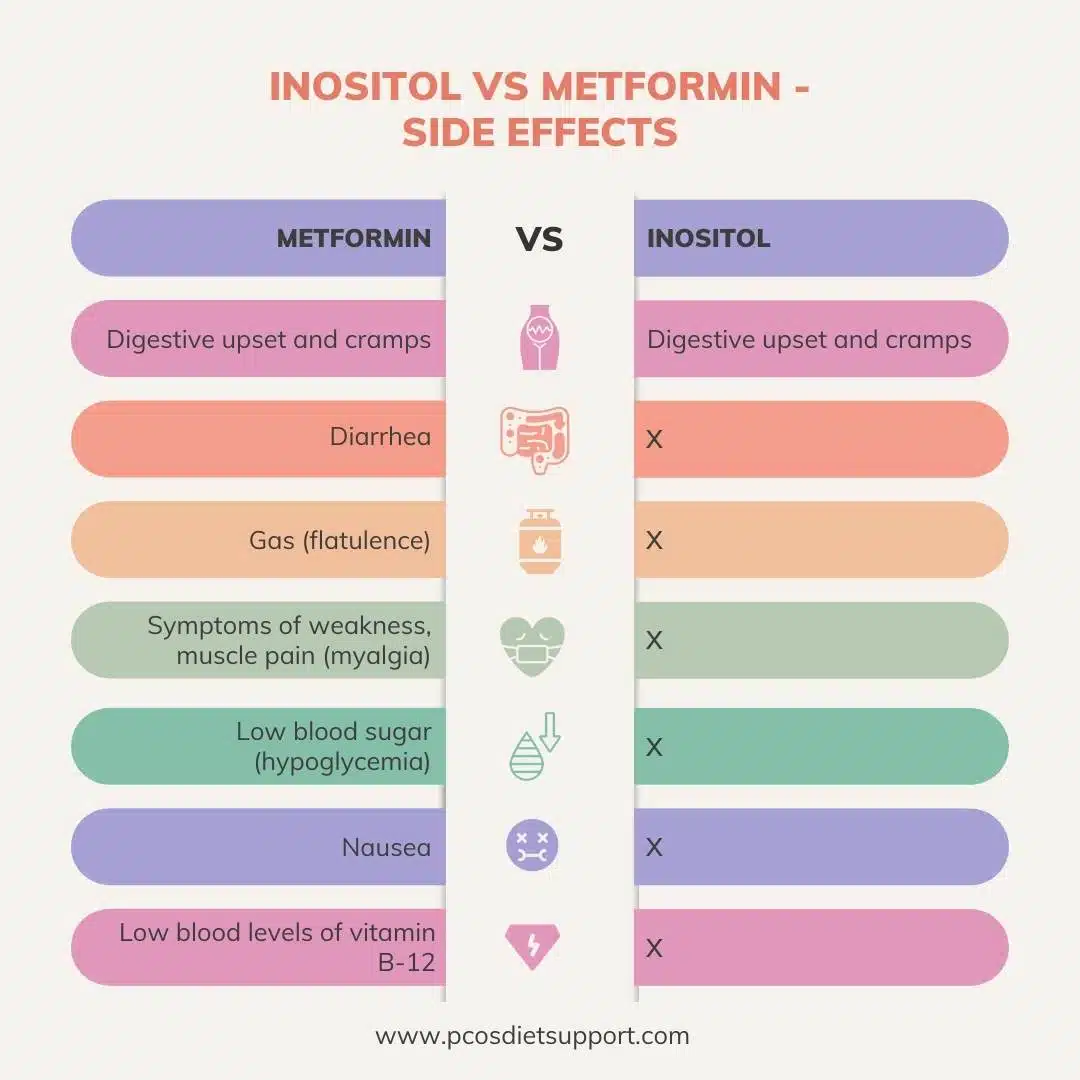
However, the pharmaceutical route is often hindered by its safety profile. Common adverse effects include significant gastrointestinal distress, such as nausea, diarrhea, and abdominal cramping. Long-term use of Metformin has also been linked to Vitamin B12 deficiency, necessitating regular monitoring and supplementation. In rare cases, it can lead to lactic acidosis, a serious metabolic complication.
Inositol: The Nutritional Signaling Pathway
Inositol, often colloquially referred to as Vitamin B8 (though it is technically a sugar alcohol), acts as a secondary messenger in insulin signaling. Within the cell, Myo-inositol (MI) and D-chiro-inositol (DCI) are responsible for different aspects of the insulin response. MI is primarily involved in the uptake of glucose from the blood, while DCI is involved in glycogen synthesis and, crucially, the regulation of androgen production in the ovaries.
In women with PCOS, a "DCI paradox" is often observed. While most tissues in the body become insulin resistant, the ovaries remain sensitive. Excessive insulin levels can cause an over-conversion of MI to DCI in the ovaries, depleting MI levels. Since MI is essential for the signaling of Follicle-Stimulating Hormone (FSH), this depletion leads to poor egg quality and disrupted ovulation.

Supplementation with a 40:1 ratio of MI to DCI—the ratio naturally found in healthy human plasma—aims to restore this balance. A 2021 systematic review and meta-analysis published in European Review for Medical and Pharmacological Sciences compared Myo-inositol and Metformin directly. The researchers concluded that Inositol was as effective as Metformin in improving insulin resistance and clinical symptoms but was significantly better tolerated by patients.
Comparative Analysis: Side-by-Side Efficacy
When analyzing the two treatments, several key metrics emerge:
1. Ovulation and Fertility
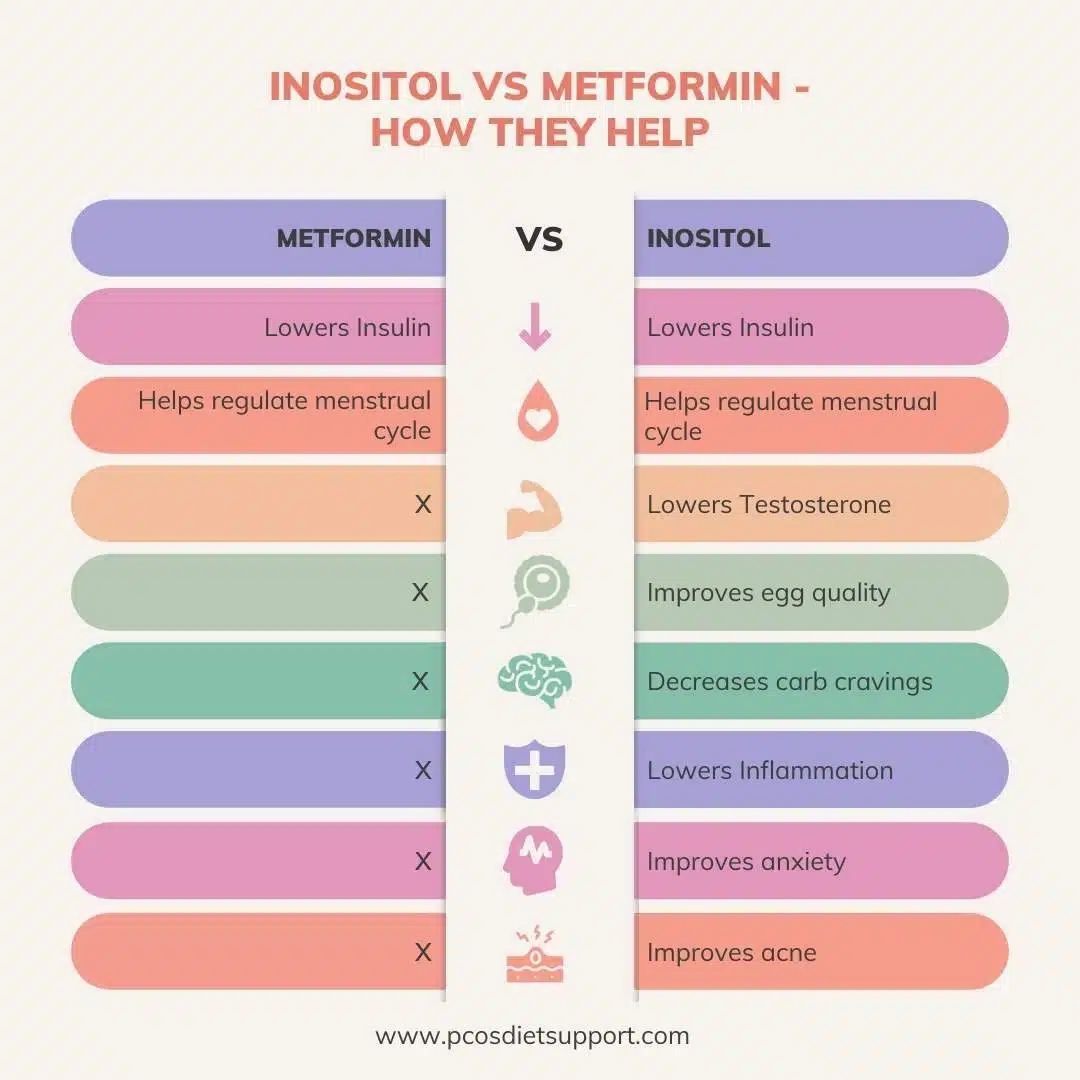
Both treatments show comparable results in restoring ovulation. However, Inositol has shown specific benefits in improving oocyte (egg) quality, which is vital for women undergoing In-Vitro Fertilization (IVF). Studies suggest that women taking Inositol require lower doses of stimulation drugs during fertility treatments.

2. Metabolic Markers
Metformin remains slightly superior in lowering fasting blood glucose levels in patients with significant hyperglycemia or pre-diabetes. Inositol, however, shows impressive results in lowering triglycerides and improving the LDL/HDL cholesterol ratio, contributing to long-term cardiovascular health.
3. Androgen Reduction
Both interventions successfully lower testosterone levels. Metformin achieves this by reducing insulin and increasing SHBG. Inositol achieves this by improving the intra-ovarian environment and correcting the insulin signaling defect at the cellular level.
4. Patient Adherence and Side Effects
This is where the two diverge most sharply. Discontinuation rates for Metformin are notably higher due to gastrointestinal intolerance. In contrast, Inositol is reported to have a side-effect profile comparable to a placebo, with only rare reports of mild nausea or headaches at very high dosages.
Medical Guidelines and Official Responses
The international medical community has begun to recognize the validity of both approaches. The International Evidence-Based Guideline for the Assessment and Management of Polycystic Ovary Syndrome, updated in 2023, continues to recommend Metformin for women with a BMI over 25 or those with high metabolic risk. However, the guidelines also acknowledge the growing body of evidence for Inositol, particularly as an alternative for those who cannot tolerate Metformin or those specifically seeking to improve fertility outcomes.
Endocrinologists frequently emphasize that these treatments are not mutually exclusive. Some clinical practitioners advocate for a "combination therapy" approach. Because Metformin and Inositol work on different parts of the insulin signaling pathway—Metformin on the liver and AMPK pathway, and Inositol on the cellular receptor signaling—they can have a synergistic effect. However, patients are warned that combined use increases the risk of hypoglycemia (low blood sugar) and must be monitored by a healthcare professional.
Broader Implications for Long-term Health
The choice between Inositol and Metformin is more than a matter of managing current symptoms; it is a preventative strategy against long-term complications. Women with PCOS face a significantly higher risk of developing Type 2 diabetes, non-alcoholic fatty liver disease (NAFLD), and endometrial cancer.
By addressing insulin resistance early through either pharmaceutical or nutritional means, patients can significantly alter their health trajectory. The shift toward Inositol represents a broader trend in medicine: the "food as medicine" movement, where naturally occurring compounds are rigorously tested against synthetic drugs. This provides patients with more autonomy and options, particularly those who prefer a "natural" approach or those whose lifestyles are incompatible with the side effects of Metformin.
Future Directions in Research
While the current data is promising, researchers call for more long-term, large-scale randomized controlled trials to determine the optimal duration of treatment and the potential for these substances to prevent gestational diabetes during pregnancy. Current studies are also exploring the role of Inositol in neurological health, as insulin resistance in the brain is increasingly linked to cognitive decline—a factor that may eventually impact aging women with a history of PCOS.
In conclusion, both Metformin and Inositol offer robust, evidence-based benefits for women struggling with the metabolic burdens of PCOS. Metformin stands as a powerful, time-tested pharmaceutical tool, while Inositol offers a highly effective, low-risk alternative that addresses the cellular root of the condition. The determination of which is "better" ultimately depends on the individual patient’s metabolic profile, fertility goals, and tolerance for side effects, highlighting the necessity for personalized, integrative care in the management of Polycystic Ovary Syndrome.
