
Polycystic Ovary Syndrome (PCOS) remains the most prevalent endocrine disorder among women of reproductive age globally, affecting an estimated 8% to 13% of the population. Central to the pathology of this condition is insulin resistance, a metabolic state that affects up to 75% of those diagnosed, regardless of body mass index. As medical practitioners and patients seek effective long-term management strategies, a significant clinical debate has emerged regarding the efficacy of two primary insulin sensitizers: the pharmaceutical agent Metformin and the nutritional supplement Inositol. While Metformin has historically served as the gold standard for off-label PCOS treatment, recent clinical trials and meta-analyses suggest that Inositol may offer comparable benefits with a significantly lower risk of adverse effects.
The Pathophysiology of Insulin Resistance in PCOS
To understand the comparative value of Inositol and Metformin, one must first examine the role of insulin in the female reproductive system. In a healthy metabolic state, insulin facilitates the uptake of glucose into cells for energy. However, in women with PCOS, cells often become resistant to these signals. The pancreas compensates by secreting higher levels of insulin, leading to hyperinsulinemia.

Excessive circulating insulin acts directly on the ovaries, specifically the theca cells, stimulating them to produce abnormally high levels of androgens, such as testosterone. Furthermore, high insulin levels suppress the production of Sex Hormone Binding Globulin (SHBG) in the liver, which further increases the amount of free, active testosterone in the bloodstream. This hormonal cascade results in the hallmark symptoms of PCOS: irregular menstrual cycles, hirsutism, cystic acne, and ovulatory dysfunction. By improving insulin sensitivity, both Metformin and Inositol aim to break this cycle, restoring hormonal balance and metabolic health.
The Pharmacological Approach: A History of Metformin
Metformin, a biguanide originally derived from the French lilac (Galega officinalis), has been a cornerstone in the treatment of Type 2 diabetes since the mid-20th century. Its application for PCOS gained traction in the 1990s as researchers identified the deep links between the syndrome and metabolic syndrome.
Metformin functions through three primary mechanisms:

- Inhibition of Gluconeogenesis: It reduces the amount of glucose produced by the liver.
- Intestinal Absorption: It slows the absorption of glucose in the gastrointestinal tract.
- Peripheral Sensitivity: It increases the sensitivity of muscle and adipose tissue to insulin, allowing for more efficient glucose uptake.
Clinical data, including a landmark study published in the Journal of Clinical Endocrinology & Metabolism, indicates that Metformin can significantly reduce fasting insulin levels and decrease androgen concentrations. Furthermore, Metformin has been associated with improved ovulation rates in women who are otherwise "clomiphene-resistant," making it a valuable tool for fertility specialists.
The Nutritional Evolution: Understanding Inositol
Inositol, often referred to as Vitamin B8 (though technically a sugar alcohol), is a naturally occurring compound found in fruits, beans, and nuts. In the human body, it serves as a "second messenger" in the insulin signaling pathway. There are nine isomers of inositol, but Myo-inositol (MI) and D-chiro-inositol (DCI) are the most relevant to PCOS management.
Inositol works by improving the "lock and key" mechanism of the insulin receptor. When insulin binds to a cell, inositol-containing phosphoglycans are released to signal the cell to open its glucose channels. Research suggests that women with PCOS often have a deficiency in these inositol-based messengers or an imbalance in the MI to DCI ratio within the ovaries. By supplementing with Inositol, patients can improve the efficiency of their existing insulin, thereby reducing the need for the body to overproduce the hormone.

Comparative Efficacy: Clinical Analysis and Data
A 2021 systematic review and meta-analysis published in European Review for Medical and Pharmacological Sciences compared the effects of Myo-inositol and Metformin on ovarian function. The findings were revealing: Inositol was found to be as effective as Metformin in improving insulin resistance, reducing androgen levels, and restoring regular ovulation.
Key data points from comparative studies include:
- Ovulation Rates: Both treatments show a significant increase in the frequency of ovulation compared to a placebo.
- Pregnancy Rates: In several trials, the pregnancy rates among women taking Inositol were slightly higher or equal to those taking Metformin, though both outperformed standard care without insulin sensitizers.
- Metabolic Markers: Metformin often shows a slight edge in reducing Body Mass Index (BMI) in certain populations, although Inositol has demonstrated superior results in improving the lipid profile (cholesterol and triglycerides).
The Side Effect Profile: A Deciding Factor
The most significant divergence between the two treatments lies in their tolerability. Metformin is notorious for its gastrointestinal side effects. Clinical reports suggest that up to 30% of patients experience nausea, abdominal cramping, diarrhea, and a metallic taste in the mouth. These symptoms are often dose-dependent and lead to a high rate of treatment discontinuation. Furthermore, long-term Metformin use has been linked to Vitamin B12 deficiency, necessitating regular monitoring and supplementation.

In contrast, Inositol is generally classified as "Generally Recognized as Safe" (GRAS) by the FDA. The side effects are rare and typically mild, such as slight nausea or headaches, which often resolve if the supplement is taken with food. This high safety profile makes Inositol an attractive first-line option for women who are sensitive to pharmaceutical interventions or those who wish to avoid the digestive distress associated with Metformin.
Chronology of Treatment Standards
The evolution of PCOS treatment has seen a shift from purely reproductive goals to holistic metabolic management:
- 1920s-1950s: Discovery and synthesis of Metformin for diabetes.
- 1990s: First major clinical trials investigating Metformin for PCOS-related insulin resistance.
- 2000s: Metformin becomes a standard off-label prescription for PCOS globally.
- 2010s: Emergence of robust clinical data regarding Myo-inositol; researchers identify the specific 40:1 ratio of MI to DCI as the physiological standard in healthy follicular fluid.
- 2020-Present: International PCOS guidelines begin to acknowledge Inositol as an experimental but promising therapy, with many practitioners now offering it as an alternative or adjunct to Metformin.
Broader Implications for Women’s Health
The comparison between Inositol and Metformin reflects a broader trend in modern medicine toward "integrative" or "functional" approaches. As patients become more proactive in managing their health, the demand for treatments with fewer side effects has driven research into nutritional compounds like Inositol.

However, medical experts caution that neither treatment is a "magic pill." The efficacy of both Metformin and Inositol is significantly enhanced when combined with lifestyle modifications, including a low-glycemic diet and regular physical activity. Furthermore, for some high-risk patients—such as those with significant obesity or a high risk of progressing to Type 2 diabetes—Metformin’s potent glucose-lowering effects may still be preferred by clinicians.
Expert Reactions and Future Directions
Leading endocrinologists suggest that the future of PCOS care may lie in combination therapy. Because Metformin and Inositol work on different parts of the insulin signaling pathway—Metformin primarily on the liver and peripheral tissues, and Inositol on the cellular receptor signaling—taking them together may yield synergistic effects. Some studies have shown that adding Inositol to a Metformin regimen allows for a lower dose of Metformin, thereby reducing side effects while maintaining clinical benefits.
As the medical community continues to gather long-term data, the consensus is shifting toward personalized medicine. A patient’s choice between Inositol and Metformin should be dictated by their specific symptoms, metabolic profile, and tolerance for side effects.
Summary of Findings
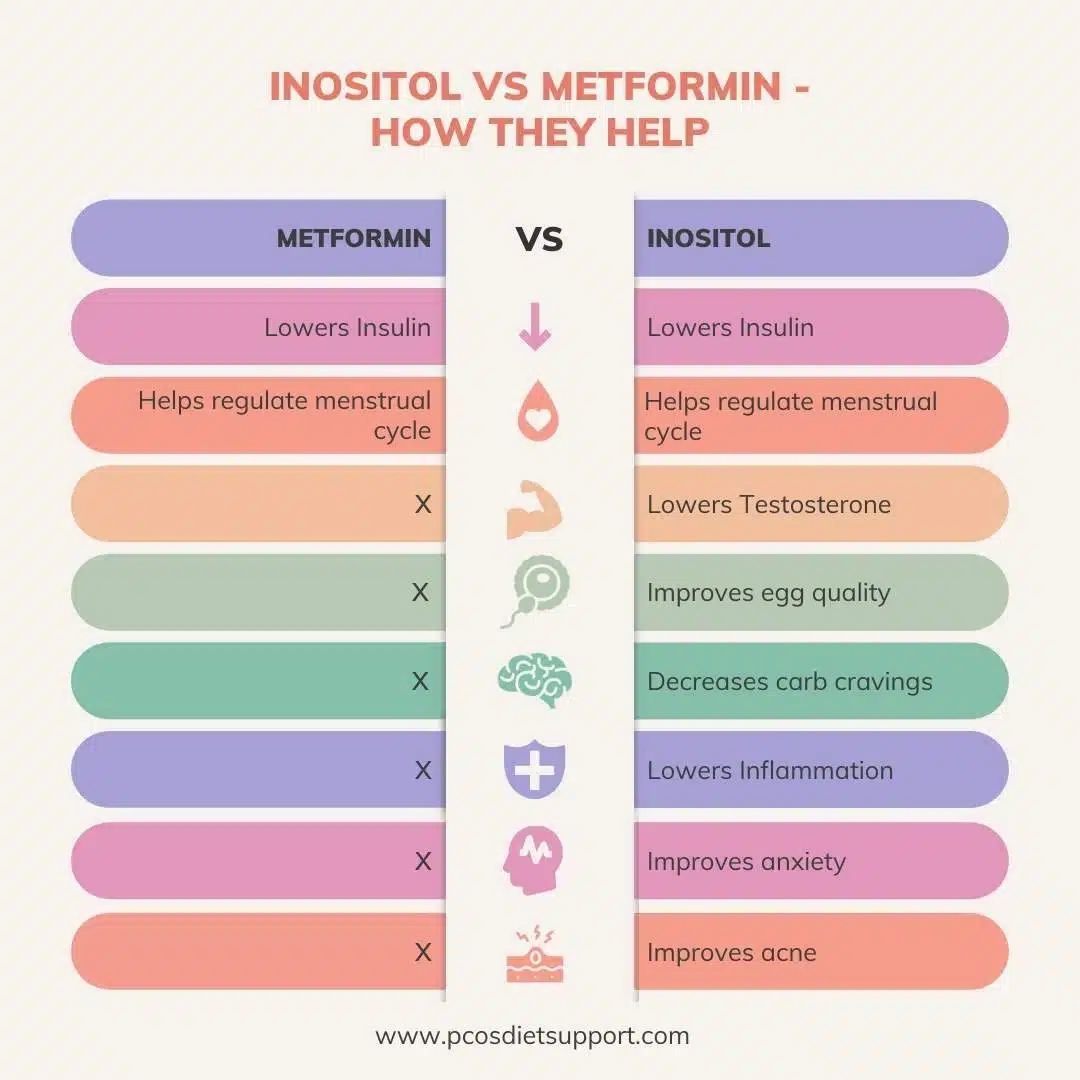
In the debate of Inositol vs. Metformin, the evidence suggests that both are powerful allies in the fight against PCOS. Metformin remains a robust, well-studied pharmaceutical option with a long history of success in metabolic regulation. Inositol, however, has emerged as a formidable challenger, offering comparable clinical outcomes in ovulation and androgen reduction with a superior safety profile. For the millions of women living with PCOS, the availability of these two distinct paths offers a hopeful outlook for managing a complex and often life-altering condition. As always, patients are advised to consult with an endocrinologist or gynecologist to determine which intervention aligns best with their reproductive and metabolic goals.