
Polycystic Ovary Syndrome (PCOS) remains the most prevalent endocrine disorder among women of reproductive age, affecting an estimated 8% to 13% of the global female population. As clinical understanding of the condition has evolved, the focus of treatment has shifted from merely addressing reproductive symptoms to managing the underlying metabolic dysfunctions that drive the disorder. Central to this management is the comparison between Metformin, a long-standing pharmaceutical staple for type 2 diabetes, and Inositol, a naturally occurring sugar alcohol that has gained significant traction in recent clinical trials. Both substances function as insulin sensitizers, yet they offer distinct mechanisms of action, side-effect profiles, and therapeutic outcomes for patients navigating the complexities of PCOS.
The Role of Insulin Resistance in PCOS Pathology
To understand the clinical utility of Metformin and Inositol, it is necessary to examine the metabolic framework of PCOS. Research indicates that up to 75% of women with PCOS exhibit some degree of insulin resistance, regardless of their Body Mass Index (BMI). Insulin resistance occurs when the body’s cells—particularly in the muscles, fat, and liver—do not respond appropriately to insulin, the hormone responsible for regulating blood glucose.

In response to this cellular "deafness," the pancreas compensates by producing excess insulin, leading to a state of hyperinsulinemia. In the context of PCOS, high levels of circulating insulin act synergistically with Luteinizing Hormone (LH) to stimulate the ovarian theca cells, causing them to overproduce androgens such as testosterone. This hormonal imbalance results in the hallmark symptoms of the syndrome: irregular menstrual cycles, hirsutism (excessive hair growth), persistent acne, and ovulatory dysfunction. Consequently, medical interventions that improve insulin sensitivity are considered foundational to PCOS care.
Metformin: The Pharmaceutical Gold Standard
Metformin has been utilized since the 1950s, originally derived from the French lilac plant, and is currently the first-line medication for type 2 diabetes. While its use for PCOS is technically "off-label" in many jurisdictions, it is widely prescribed by endocrinologists and gynecologists to address the metabolic facets of the condition.
Mechanisms of Action
Metformin primarily targets the liver and the gastrointestinal tract to lower circulating glucose and insulin levels through three distinct pathways:

- Inhibition of Gluconeogenesis: It suppresses the liver’s production of glucose, ensuring that baseline blood sugar levels remain stable.
- Enhanced Insulin Sensitivity: It increases the sensitivity of muscle cells to insulin, allowing for more efficient glucose uptake and utilization.
- Reduced Intestinal Absorption: It slows the rate at which the body absorbs glucose from the digestive system into the bloodstream.
Clinical Efficacy and Benefits
Decades of randomized clinical trials have validated Metformin’s ability to lower androgen levels and restore more regular menstrual cycles. Furthermore, Metformin has been associated with a reduction in the risk of developing gestational diabetes in women who conceive. While often associated with weight loss in diabetic populations, its effect on BMI in women with PCOS is frequently described as modest, with some studies showing little to no significant weight reduction without concurrent lifestyle interventions.
Inositol: The Emerging Nutritional Intervention
Inositol, specifically in the forms of Myo-inositol (MI) and D-chiro-inositol (DCI), is a carbocyclic sugar found in fruits, beans, grains, and nuts. In the human body, inositols act as "second messengers" in the insulin signaling pathway. When insulin binds to its receptor on a cell wall, inositol-containing molecules are released to relay the signal into the cell, triggering glucose uptake.
The Logic of Supplementation
In women with PCOS, there is often a deficiency in the enzymes that convert Myo-inositol to D-chiro-inositol, or an overall depletion of inositol levels in the follicular fluid. This deficiency impairs the insulin signal, contributing to the cycle of insulin resistance. Supplementation aims to restore these levels, thereby "greasing the wheels" of the insulin receptor.

Scientific Advancements in Inositol Research
A 2021 systematic review and meta-analysis published in European Review compared the effects of Myo-inositol and Metformin directly. The findings suggested that Myo-inositol was comparable to Metformin in its ability to improve insulin resistance, lower androgen levels, and restore ovulation. Notably, Inositol has shown specific promise in improving oocyte (egg) quality, a factor that is critical for women undergoing fertility treatments like In Vitro Fertilization (IVF).
Comparative Analysis: Side Effects and Patient Tolerance
The primary differentiator between these two interventions often lies in patient adherence and tolerance. Metformin is notorious for its gastrointestinal side effects. Clinical data suggests that a significant percentage of patients experience nausea, abdominal cramping, diarrhea, and a metallic taste in the mouth. These symptoms are often dose-dependent and can be so severe that patients discontinue the medication. Furthermore, long-term Metformin use has been linked to Vitamin B12 deficiency, necessitating regular monitoring and supplementation.
In contrast, Inositol is generally classified as "Generally Recognized as Safe" (GRAS) by the FDA. Side effects are rare and typically limited to mild digestive upset or occasional headaches when taken in very high doses. This high safety profile makes it an attractive option for women who cannot tolerate the pharmacological intensity of Metformin.

Chronology of Clinical Adoption
The integration of these treatments has followed a distinct timeline:
- 1990s: Metformin begins to be used off-label for PCOS as the link between insulin and androgens is solidified.
- Early 2000s: The first major studies on Myo-inositol emerge, primarily out of Italy, showing its potential for restoring ovulation.
- 2013-2015: Research identifies the importance of the 40:1 ratio of Myo-inositol to D-chiro-inositol, mimicking the natural ratio found in human plasma.
- 2018-Present: Major international PCOS guidelines begin to acknowledge inositol as an experimental but promising therapy, while Metformin remains the primary recommendation for metabolic health.
Supporting Data: Head-to-Head Outcomes
When examining the clinical data, the choice between the two often depends on the patient’s specific goals.
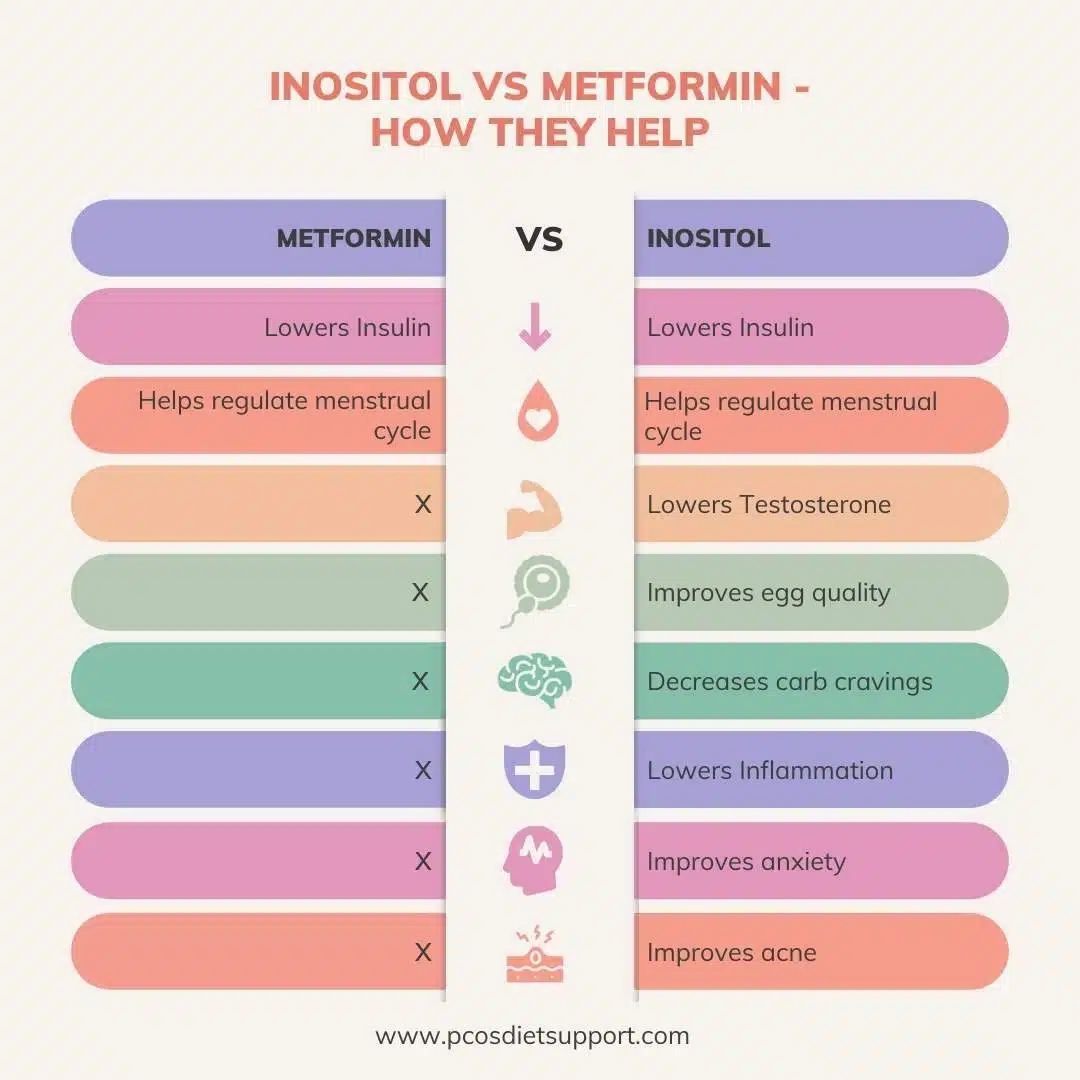
| Feature | Metformin | Inositol (Myo/D-Chiro) |
|---|---|---|
| Primary Goal | Metabolic/Diabetes Prevention | Fertility/Symptom Management |
| Androgen Reduction | Significant | Significant |
| Ovulation Restoration | Moderate to High | High |
| Weight Loss Impact | Modest | Modest |
| Side Effect Risk | High (GI Distress) | Very Low |
| Accessibility | Prescription Required | Over-the-Counter |
Research published in PubMed Central highlights that while Metformin is superior in suppressing hepatic glucose production, Inositol may have a more targeted effect on the ovaries themselves, potentially making it more effective for those specifically seeking to improve fertility and egg quality.

Official Responses and Medical Consensus
The medical community’s stance is currently one of cautious optimism regarding Inositol. Organizations such as the American College of Obstetricians and Gynecologists (ACOG) and the Endocrine Society continue to recognize Metformin as a validated tool for managing the metabolic complications of PCOS, such as impaired glucose tolerance.
However, many reproductive endocrinologists have begun integrating Inositol into their protocols. Dr. Angela Grassi, a leading dietitian specializing in PCOS, notes that the three-fold action of Metformin on the liver, muscles, and gut provides a robust metabolic defense, but the "lock and key" mechanism that Inositol supports at the cellular receptor level is equally vital. The consensus suggests that these two treatments are not necessarily mutually exclusive; in some cases, they are prescribed together to provide a synergistic effect, though this requires careful medical supervision to prevent hypoglycemia (low blood sugar).
Broader Impact and Implications for Long-term Health
The debate between Inositol and Metformin reflects a broader shift in women’s healthcare toward personalized medicine. As PCOS is a lifelong condition, the long-term implications of treatment are paramount.
For many women, the choice is driven by lifestyle. Metformin offers a rigorously tested, low-cost pharmaceutical option that is often covered by insurance. For others, the natural origin and low side-effect profile of Inositol represent a more sustainable long-term approach to managing a chronic hormonal imbalance.
The implications for the healthcare system are also significant. With PCOS being a major precursor to type 2 diabetes and cardiovascular disease, effective management in early adulthood can prevent billions of dollars in future healthcare costs. Whether through the pharmaceutical pathway of Metformin or the nutraceutical pathway of Inositol, the goal remains the same: restoring metabolic homeostasis and improving the quality of life for millions of women worldwide.
As research continues to evolve, it is expected that future clinical guidelines will provide more definitive dosing and ratio recommendations for Inositol, potentially elevating it from a "supplement" to a standardized treatment alongside Metformin. For now, the medical advice remains consistent: patients should consult with their healthcare providers to determine which insulin sensitizer aligns best with their metabolic profile, reproductive goals, and tolerance for side effects.